-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2017; 7(1): 11-13
doi:10.5923/j.ajmms.20170701.03

Our Experience Videoendoscopic Adrenalectomy in Patients with Benign Adrenal Tumors Large Sizes
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKarimov Shavkat Ibragimovich, Berkinov Ulugbek Bazarbaevich, Sahiboev Dilshod Parpijalilovich
Tashkent Medical Academy, Uzbekistan
Correspondence to: Sahiboev Dilshod Parpijalilovich, Tashkent Medical Academy, Uzbekistan.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Presenting the results of laparoscopic adrenalectomy in 15 patients benign tumors of the adrenal glands that are larger than 5 cm. We compare the duration of operations, the frequency of complications and postoperative course. Also highlighted in particular surgical technique when performing these operations. A comparative analysis of the results in the study group and the control group, which accounted for 82 patients who underwent laparoscopic adrenalectomy at the size of the tumor less than 5 cm.
Keywords: Benign adrenal tumors, Big size, Laparoscopic adrenalectomy
Cite this paper: Karimov Shavkat Ibragimovich, Berkinov Ulugbek Bazarbaevich, Sahiboev Dilshod Parpijalilovich, Our Experience Videoendoscopic Adrenalectomy in Patients with Benign Adrenal Tumors Large Sizes, American Journal of Medicine and Medical Sciences, Vol. 7 No. 1, 2017, pp. 11-13. doi: 10.5923/j.ajmms.20170701.03.
- Presenting the results of laparoscopic adrenalectomy in 15 patients benign tumors of the adrenal glands that are larger than 5 cm. We compare the duration of operations, the frequency of complications and postoperative course. Also highlighted in particular surgical technique when performing these operations. A comparative analysis of the results in the study group and the control group, which accounted for 82 patients who underwent laparoscopic adrenalectomy at the size of the tumor less than 5 cm.
1. Relevance
- Currently, laparoscopic adrenalectomy (LAE) is the gold standard in patients with benign tumors of the adrenal glands. LAE has all the advantages of minimally invasive operations, and creates the opportunity to perform an adequate level of operation [1]. According to various authors, the main factor affecting the ability to perform LAE, is the size of a tumor of the adrenal gland. For several years, it was believed that a tumor of the adrenal gland that is larger than 5 cm, is a contraindication to perform LAE [2], establishes that the large size of the tumor followed by large anatomy changes in the adrenal gland, which leads to difficulties in the identification of anatomical structures. The value of this fact is reflected in increased incidence of perioperative complications and access conversion and increase in the critical time spent on performance of LAE [3]. And with an increase in the size of tumors of the adrenal glands, a regular increase in the probability of malignant process and was considered a contraindication to perform LAE [4].However, recently put into practice a more informative diagnostic methods, such as CT and MRI, and it has greatly improved the topical diagnosis of adrenal tumors, which made it possible to specify before the operation idea of the features of the area of the adrenal gland and the opportunity to facilitate the identification of anatomical structures in during surgery [5, 6]. Another important aspect is the improvement of anesthesia, which allows for longer operation while maintaining the same level of safety of anesthesia for patients [7]. In view of the above points, there is evidence in the literature on the successful implementation of LAE with adrenal tumors larger than 5 cm. According to S.I. Emelyanov et al. LAE with adrenal tumors ranging in size from 51 to 87 mm, is the operation of choice in this group of patients subject to these requirements to the realization of the given intervention [8]. R. Sharma et al. [9] and G. Zografos et al. [10] reported the laparoscopic removal of adrenal tumors at a rate of 8-9 cm in 15 patients. According to other authors, the maximum size of an adrenal tumor, laparoscopic successful remote access up to 12 cm [11].
2. Objective
- To study the possibility of laparoscopic adrenalectomy in patients with benign tumors of the adrenal glands in size greater than 5 cm.
3. Material and Methods
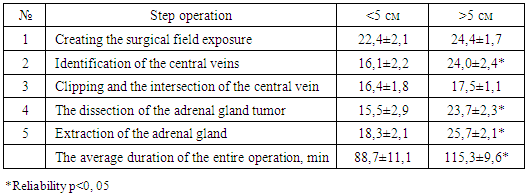
- Our experience LAE with adrenal tumors is 97 operations. For the diagnosis of adrenal tumors was used complex laboratory and instrumental studies, including CT proved more informative. All patients were divided into 2 groups. All patients were produced by LAE lateral transabdominal approach. Preference lateral transabdominal laparoscopic approach gave in connection with the fact that it best meets the criteria for evaluating the spatial surgical approaches. The first group included 15 patients who had an adrenal tumor size greater than 5 cm. Right side LAE was performed in 10 (66.6%) patients and left-sided LAE - 5 (33.3%). Diameters of remote tumors ranged from 51 to 98 mm with right LAE and 52 to 75 mm - in the left LAE. The average tumor size in this group was 71 ± 8 mm.The second group consisted of 82 patients who had adrenal tumors smaller than 5 cm. In this group right-sided tumor was detected in 37 (45.1%) patients, and left-sided - in 45 (54.9%) patients. The average size of the tumor in the second group was 34 ± 11mm.By morphological character of tumor patients were divided as follows: a mixed structure adenoma - 5 and 43, aldosteronoma - 3 and 13, pheochromocytoma - 3 and 3, nodular adrenocortical hyperplasia - 0 and 6 and adrenal cyst - 4 and 2, respectively.Preoperative preparation of patients depended largely on the nature of the tumor, and the patient was placed on an operating table in the supine position on the side opposite to the side of the lesion. Pneumoperitoneum procedure was applied for the safe and the gas pressure in the peritoneal cavity does not exceed 10 mm Hg during surgery. The main stages of the operation by increasing the adrenal tumor size remained the same and included the creation of the exposure of the surgical field, the central vein authentication, clipping and the intersection of the central vein, dissection of the adrenal gland in a single unit with tumor extraction macropreparations. All macropreparations (Fig. 1 and Fig. 2) after surgery is compulsory for histological examination.
 | Figure 1. Tumor of the right adrenal gland (pheochromocytoma) dimeters 77x52 mm |
 | Figure 2. Tumor of the right adrenal gland (adenoma) dimensions 33x27 mm |
|