-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2016; 6(6): 193-196
doi:10.5923/j.ajmms.20160606.06

Acute Obstructive Ileus as a Late Postoperative Complication of Peptic Ulcer Disease
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLM. Sh. Khakimov, U. K. Nasritdinov, Sh. E. Ashurov, D. Khusinov
Department of Faculty and Hospital Surgery, Tashkent Medical Academy, Tashkent, Uzbekistan
Correspondence to: M. Sh. Khakimov, Department of Faculty and Hospital Surgery, Tashkent Medical Academy, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Objective: To improve the results of surgical treatment of patients with acute intestinal obstruction caused by phytobezoars. Material and Methods: A retrospective analysis of the results conducted by the treatment of 60 patients with acute intestinal obstruction, caused by phytobezoars who were hospitalized in the 2 - clinic of the Tashkent Medical Academy from 2005 to 2015. It should be noted that phytobezoars occurred mainly in patients who previously underwent surgery for complications of gastric and duodenal ulcers. Results: 12 patients (20%), intestinal obstruction were resolved conservatively. The rest underwent operations. Patients who have surgery performed on the small intestine, for the purpose of decompression were set nasoenteral tube, which was removed on 2-3 days after operation. Postoperatively developed the following complications: postoperative wound seroma (2 cases), festering wound (1 case), postoperative pneumonia (2 patients), which were cropped with conservative therapy. One patient on the 2nd postoperative day developed intestinal obstruction, which resolved conservatively. Length of hospital stay were from 6 to 9 days. No deaths were observed. Conclusions: Acute intestinal obstruction caused by phytobezoars meets several times more common in people undergoing surgery for peptic ulcer disease and its complications. It should be noted that most of these patients had no capability information about phytobezoars after such surgical interventions. The diagnostic algorithm is necessary to include endoscopy for diagnosis of gastric bezoar and assess the possibility of its endoscopic removal.
Keywords: Acute intestinal obstruction, Phytobezoars, Ulcer complications, Endoscopy
Cite this paper: M. Sh. Khakimov, U. K. Nasritdinov, Sh. E. Ashurov, D. Khusinov, Acute Obstructive Ileus as a Late Postoperative Complication of Peptic Ulcer Disease, American Journal of Medicine and Medical Sciences, Vol. 6 No. 6, 2016, pp. 193-196. doi: 10.5923/j.ajmms.20160606.06.
1. Introduction
- Acute obstructive ileus occupies a considerable proportion of urgent pathologies. However, the main causes of this disease in these patients after operations on the stomach for peptic ulcer disease are bezoars of various origins [1, 2, 3, 8].Bezoars (from French -. bezoard) - is a rare foreign bodies if gastrointestinal tract, formed from various non-digested components that have a feature imperceptibly increase in volume during the time. There are several kinds of bezoar: phyto-, tricho-, sebo- (from certain types of fat), hemato- (blood clots), litho- (clay, chalk, lime), pseudo- and polibezoars. Among them, more than 80% accounted for by phytobezoars [1-3, 5, 8]. They are formed from plant fiber, seed and persimmon fruit, hawthorn, pitted cherries, grapes, wild plums, figs, etc. Depending on the duration of the existence of consistency can be up stony hardness, can be single or multiple, and the size can reach up to the size of the internal organ. Phytobezoars rank third place among causes of acute obstructive ileus after adhesions and tumor genesis [1, 2]. Most often phytobeozars formed in patients after gastric resection for complications of peptic ulcer disease [2]. According to G. Miller (2014) after resection of the stomach, they are found in 0.4%, and after vagotomy - in 7.4% of patients. According to many authors, in the pathogenesis of forming phytobezoars more common in these patients plays a big part of the large fistula between the stomach and intestine, the lack of the pyloric sphincter, which provides regulation of the passage of food, reduced level of acidity and pepsine enzymes of the stomach and small volume. It explains that after above mentioned operations production of pepsine by stomach rapidly decrease. Pepsine is an enzyme and contains in stomach fluid, digest proteins of food. A lack of production of pepsine leads to forming bezoars after eating some products. An important role is played by catarrhal or atrophic gastritis, developing after the above operations and the emergence of fungal flora, which contributes to the appearance of thick mucus in the lumen of the stomach [1-3, 6-8].Currently, there are several methods for the treatment of acute obstructive ileus due phytobezoars. Among them, widespread lavage method, endoscopic crushing removing bezoar and open or laparoscopic surgery. The choice of treatment depends on the unit location, size, origin, and the density of the bezoar [7, 8].
2. Material and Methods
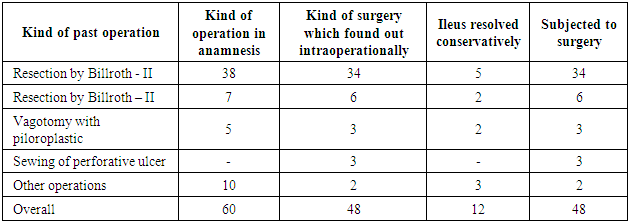
- We performed a retrospective analysis of treatment of 60 patients with gastrointestinal bezoar, who were hospitalized in the second clinic of the Tashkent Medical Academy from 2005 to 2015. Tashkent Medical Academy is situated in Tashkent, capital of the Republic of Uzbekistan. Women were 28 men - 32. The age of patients ranged from 25 to 62 years, average age was 37,5±2,5 (men age from 25 to 62, women – 28 to 61). All patients received in the autumn and spring periods with symptoms of acute intestinal obstruction in the period from 2 to 48 hours of the disease.In anamnesis, to 38 patients were performed resection of stomach by Billroth-II of, to 7 – by Billroth-I, to 5 - pyloroplasty with vagotomy, 10 patients did not know about the kind of the past operation. Onset 37 (61.5%) patients was associated with intake of hawthorn fruit, 6 (10%) - with quince and pomegranate seeds, 3 (5%) - a banana. 14 (23.5%) patients denied the link between the onset of the disease from taking any fruit. Phytobezoars were found out during surgery.In 12 (20%) patients having acute obstructive ileus was resolved by conservative measures, in the remaining 48 (80%) cases, the patients were subjected to surgical intervention (Table 1).
|
|

3. Results
- The introduction of patients with acute intestinal obstruction was conducted according to the existing medical diagnostic standard emergency surgical pathology. In 20% (12 patients) cases of bowel obstruction was resolved with conservative measures. For this, we took to patients infusions which content Glucose with Kalium chloride, intramuscularly M-cholinomimetic Proserine and peroral laxative Duphalac. The rest of the patients were subjected to surgery. When performing surgery on the small intestine in all patients with the aim of bowel decompression was set nasoenteral tube, which was removed at 2-3 postoperative day.Postoperatively developed the following complications: postoperative wound seroma (2 cases), festering wound (1 case), postoperative pneumonia (2 patients). After conservative therapeutic measures these complications were licvidated. One patient on the 2-nd postoperative day developed intestinal obstruction. After conservative therapy with prolonged epidural anesthesia ileus resolved. Length of hospitalization were from 6 to 9 days. No deaths were observed.In the late period in 1 case (patient with festering wounds) developed postoperative ventral hernia, which required planning operation.
4. Discussion
- Nowadays there are different approaches to the treatment of acute obstructive ileus, the cause of which are phytobezoars.Researchers Katharine E, Marsha K. (2012) report that they have used the following methods: lavage, endoscopy with or without crushing bezoar, laparoscopic and open surgery. Lavage method allows authors to resolve the acute intestinal obstruction up to 50% of cases, and endoscopic - improves efficiency by 5-10%. The ineffectiveness of the above methods is an indication for laparoscopic or videoassisted bringing down of phytobezoars. Open surgery is used when it is impossible to eliminate the acute intestinal obstruction or the presence of minimally invasive indications of nasoenteral decompression [7].Fu-Chin Hung et al. (2013) report on the effective application of highly carbonated beverage Coca-Cola in giant stomach phytobezoars. If its efficacy in this disease is up to 50%, the combined use of it with the endoscopic method allows eliminate phytobezoars up to 90% of cases. Indications for endoscopic removal phytobezoars sizes are last no more than 3.0 cm. For larger sizes the authors recommend to perform endoscopic fragmentation of phytobezoars with following remove. Large bezoars that cannot be crushed, it is advisable to remove by laparoscopic or open methods [8]. According to these authors observed relapse phytobezoars to 14% of cases. In order to prevent the disease is necessary to restrict or prohibit the patients who underwent resection of the stomach and other palliative surgery for peptic ulcer disease, the adoption of the fruit with a high content of fiber and tannin.Dirican A. et al. (2014) retrospectively studied the results of surgical treatment of acute obstructive intestinal obstruction caused by phytobezoars in 24 patients. Among these, 80 had a history of surgery for peptic ulcer disease. Researchers have noted an important role of MSCT in the diagnosis of the causes of obstruction. Of the 9 patients in 7 cases failed in the preoperative period to establish an accurate diagnosis of the etiological and topical. All patients were subjected to surgery: laparoscopic relegation bezoar in the large intestine - 1 relegation phytobezoars manually - 11, through the removal of enterotomy - 12 observations. During surgery, 2 patients were diagnosed gastric bezoar, which may be removed by endoscopy. The authors argue whether to include endoscopy in the diagnostic algorithm of acute intestinal obstruction in patients who underwent surgery for peptic ulcer disease or has the disease history.1 patient before surgery bezoar stomach and small intestine were detected on MSCT. This diagnostic method is considered to be valuable and gives complete information about the location of bezoar in the gastrointestinal tract. But the possibility to carry out this type of study for all it was not because of the high cost of the method. Besides, we think that informational content of MSCT lower in patients who have pneumatosis of intestine. Endoscopic removal attempt was unsuccessful due to the increased density of bezoar, and therefore made gastrotomy. The researchers said the development of postoperative complications in patients who opened the lumen of the stomach or intestines. Lavage methods did not use [9].
5. Conclusions
- Analysis of their own clinical material and literature data led to the following:1. Acute intestinal obstruction caused by phytobezoars meets several times more common in people undergoing surgery for peptic ulcer disease and its complications. It explains that after those operations production of pepsine by stomach rapidly decrease. Pepsine is an enzyme, which contain in stomach fluid and digest proteins of food. A lack of production of pepsine leads to forming bezoars after eating some products. It should be noted that most of these patients had no capability information of phytobezoars after such surgical interventions. This dictates the feasibility of the recommendations of the fruit limitations with high fiber content prior to discharge this patient population.2. To diagnostic algorithm it is necessary to include endoscopy for diagnosis of gastric bezoar and assess the possibility of its endoscopic removal.3. With the ineffectiveness of lavage and endoscopic methods of treatment, it is advisable to start the surgery with laparoscopy and laparoscopic attempts at bringing down bezoar or using minimal access.