-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2016; 6(4): 123-128
doi:10.5923/j.ajmms.20160604.01

Birth Preparedness and Complication Readiness among Women Attending Antenatal Care Clinic in Health Facilities within Bureti Sub County of Kericho County, Kenya
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLPhanice K. Omari1, Yaw A. Afrane2, Peter Ouma3
1Department of Environmental Health Sciences, University of Kabianga, Kericho, Kenya
2Department of Microbiology, University of Ghana Medical School, Legon, Ghana
3KEMRI/CDC Public Health Program, Village Market, Nairobi, Kenya
Correspondence to: Phanice K. Omari, Department of Environmental Health Sciences, University of Kabianga, Kericho, Kenya.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Maternal mortality remains a major public health problem in Kenya with 488 deaths per 100,000 live births. Birth preparedness and complication readiness is one of the recommended strategies by the major global initiatives and implemented by the Kenyan government to reduce maternal mortality. It is the process of planning for normal birth and anticipating the actions needed in case of an emergency during pregnancy, delivery and post partum period. Studies conducted among the urban Kenyan women have found a higher proportion of women to be prepared for birth and associated complications. However, little is known about the status of Birth Preparedness and Complication Readiness of pregnant women in rural regions. The study aimed at assessing Birth Preparedness and Complication Readiness among women attending antenatal care clinic (ANC) at health facilities within Bureti Sub County. A facility based cross-sectional study was carried out among pregnant women attending health facilities within the Sub County. Results from 149 respondents showed that large proportion of the women 70.5% (n=105) were prepared for birth while 90.6% (n=135) reported readiness for complications. Majority of the respondents 87.9% (n= 131) had identified a place of delivery, 72.5% (n=108) knew the expected date of delivery. Only 4.7% of the respondents were able to mention at least two danger signs in all the three phases namely pregnancy, delivery, and post partum. Vaginal bleeding was most mentioned danger sign in all the three phases. Women who recognized vaginal bleeding as a danger sign in pregnancy were 3 times more likely to be prepared for birth than those who did not know (OR=3.00, CI 1.43-6.16, p<0.005). Knowledge of vaginal bleeding was also associated with complication readiness (OR=3.47, CI 0.007-5.42, p<0.005). The study revealed that a greater proportion of women attending ANC clinic within Bureti Sub County were well prepared for birth and ready for obstetric complications. However, the low awareness of obstetric danger signs may lead to the first and second delays in seeking health care during obstetric emergencies. It is therefore important for the ministry of health to intensify ANC health education on obstetric danger signs to all women attending ANC irrespective of their demographic characteristics so as to increase their knowledge on obstetric danger signs.
Keywords: Birth Preparedness, Complication Readiness, Maternal Mortality, Ante-natal Care, Kenya
Cite this paper: Phanice K. Omari, Yaw A. Afrane, Peter Ouma, Birth Preparedness and Complication Readiness among Women Attending Antenatal Care Clinic in Health Facilities within Bureti Sub County of Kericho County, Kenya, American Journal of Medicine and Medical Sciences, Vol. 6 No. 4, 2016, pp. 123-128. doi: 10.5923/j.ajmms.20160604.01.
Article Outline
1. Introduction
- Maternal mortality continues to be a major public health challenge in the 21st century. The World Health Organization (WHO) estimates that 830 women die daily from pregnancy and childbirth related causes. Of the deaths, ninety nine percent occur in developing countries where the burden is grater in rural and poor communities [1]. In Kenya, the maternal mortality is currently standing at 488 deaths per 100,000 live births [2]. These figures are very high compared to Kenya’s target towards achieving millennium development goal number 5(MDG 5) which is at 147 deaths per 100,000 live births by 2015 [3]. Ante Natal Care/Focused Ante Natal Care is one of the strategies recommended by WHO to reduce maternal mortality, the strategy is actively implemented by the Kenyan government [4]. Birth Preparedness and Complication Readiness (BPCR) is a component of Focused Ante Natal Care (FANC). It is the process of planning for normal birth and anticipating the actions needed in case of an emergency during pregnancy, delivery and post partum period. It is the initial prerequisite step to seek skilled birth attendance, during delivery and also when there is an obstetric emergency [5]. Therefore, BPCR addresses the delay in deciding to seek care and the delay in reaching healthcare care facility [6]. A birth plan should be discussed on the first visit, reviewed in subsequent visits and finalized by 32 weeks during Ante Natal Care [7]. A birth and emergency preparedness plan includes identification of the following elements; knowing danger signs of obstetric complications and emergencies, choosing a preferred place of birth, saving money to cater for birth related and other emergency care, making arrangements for transport and identifying a decision maker in case of an emergency. Other aspects of birth preparedness include the knowledge of expected date of delivery, labor signs and importance of postnatal care [8]. The danger signs in pregnancy are vaginal bleeding, severe headache, blurred vision, anemia, swelling of hands and face, difficulty in breathing, fits, fever, and reduction or absent foetal movement and drainage of liquor. Major danger signs during labor and childbirth include severe vaginal bleeding, prolonged labor (more than 12 hours), convulsions and retained placenta. Whereas danger signs during the postpartum period include; severe vaginal bleeding, fits, engorged breasts, foul-smelling vaginal discharge, and fever [9].BPCR improves utilization of skilled care as demonstrated in Western Kenya [10], Uganda [11], Tanzania [12], and Burkina Faso [13]. Cost of emergency care and transport which are barriers in accessing skilled care [5] are addressed in birth preparedness. In Kenya, 92% of women sought antenatal care while deliveries by skilled birth attendants in the year 2009 were at 44% [2]. Information about birth preparedness and complication readiness in rural areas in Kenya is not well documented.In June, 2013, the Kenyan government introduced free maternal and child health services to all public health facilities. This has remarkably improved maternal health, as most mothers now deliver under skilled care. Community health strategy has also contributed to assess of maternal health services [13]. A study carried out at Kenyatta National hospital, Kenya showed that only 6.7% of the pregnant women attending ANC clinic knew three or more danger signs and all respondents were unable to identify danger signs which indicate severe pre-eclampsia and eclampsia. 55% had made prior arrangement for transport and large proportion of clients was not prepared for obstetric emergencies [14] Few studies of this nature have been done in rural areas of Kenya. The purpose of this study was to assess the level of birth preparedness and complication readiness and associated factors among women attending antenatal care clinic at the health facilities within Bureti Sub County, Kericho County, Kenya.
2. Materials and Methods
- The study was carried out from November 2014 to January 2015 in Bureti Sub County, one of the 5 Sub Counties of Kericho County in the Rift valley region of Kenya. The Sub County lies 0025’, 0043’ S, and 350 05’, 36035’ E. It has an area of 806 Km2 and is sub divided into four administrative divisions with total population of 182,061 persons. The Sub County is largely inhabited by the Kipsigis ethnic group, who earn their living through small scale subsistence farming, trade and cash crop farming mainly tea. The Sub County has two level 4 health facilities, three level 3 health facilities and twenty four level 2 health facilities.Descriptive cross-sectional study design was adopted for this study, all facilities in the Sub County were entered into Ms Excel according to their levels and then a random selection was done. One facility was randomly selected from each of the three levels i.e. level 2, level 3 and level 4. The number of participants chosen per facility was proportional to its average monthly workload. All pregnant women coming for the second visit and above were enrolled to participate in the study. A sample size of 149 respondents was taken.A semi-structured questionnaire was designed, pre-tested and used to collect information on demographic characteristics, birth preparedness practices, complication readiness practices and knowledge of obstetric danger signs. An exit interview was conducted with the help of trained research assistants. Data was entered into Ms Access database 2007 and analyzed using Statistical Package for Social Sciences (SPSS Version 16) computer program. Social and demographic characteristics were summarized by frequencies and percentages. Binary logistic regression was used to determine association between socio-demographic factors and birth preparedness and complication readiness. The results were presented as odds ratios (OR) with 95% confidence intervals (CI). All tests were 2 sided and considered statistically significant at p<0.05.The study was approved by the Jaramogi Oginga Odinga University of Science and Technology Board of Post Graduate Studies, ethical clearance was obtained from the University of East Africa Baraton Ethical Review Committee. Permission to conduct the study was sought from the Sub County Medical officer of Health - Bureti Sub County and all Officers In-charge of participating health facilities. Written informed consent was sought from all research participants after explaining the purpose, procedure, benefits and discomforts the study entails. Participants were also informed of the right to refuse to participate in the study or to withdraw consent to participate at any time without reprisal. Confidentiality of research data was ensured.
3. Results
3.1. Demographic Characteristics of Respondents
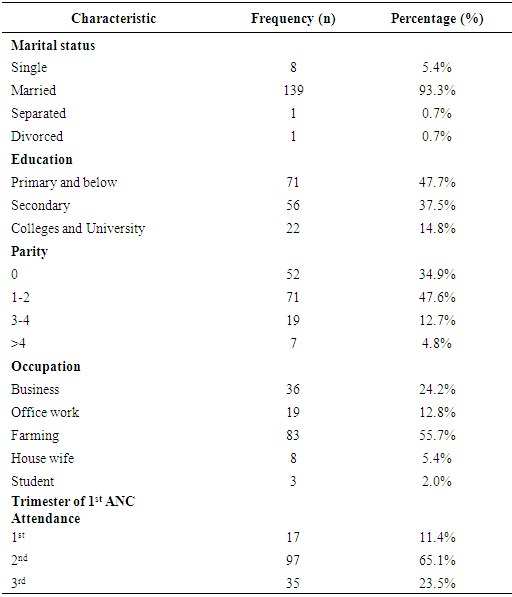
- A total of 149 women who were attending ANC clinic for the second visit were interviewed. The mean age of the respondents was 24.5 years, with a range of 18-43 years. Majority of the respondents 93.3% (n=139) were in a matrimonial union, those who had attained primary school education and below were 47.7% (n=71). Farming was the most common occupation of the respondents at 55.7% (n=83). The highest parity was 10 while those expecting their first child were 34.9% (n=52). Only 11.4% (n=17) of the respondents had initiated their ANC attendance within the first trimester (Table 1).
|
3.2. Birth Preparedness and Complication Readiness Practices
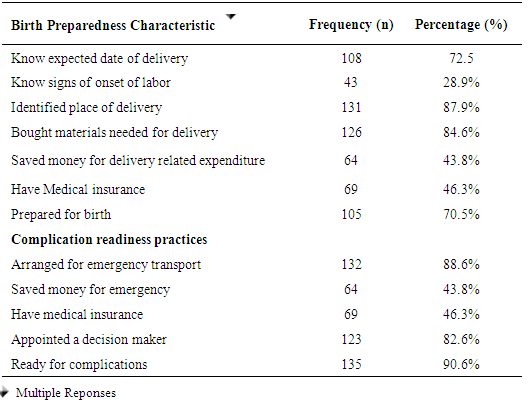
- Table 2 shows birth preparedness practices and complication readiness among the women attending ANC clinics within Bureti Sub County. A larger proportion of the women 70.5% (n=105) were prepared for birth. Regarding individual birth preparedness practices; majority of the respondents 87.9% (n= 131) had identified a place of delivery, 72.5% (n=108) knew the expected date of delivery but only 28.9% (n=43) knew the signs of onset of labor. A higher percentage of women 84.6% (n=126) had bought materials needed for delivery. A higher proportion of women 81.9% (n=122) had made arrangement for transport to the health facility at birth. Nearly half 46.3% (n=63) of the women interviewed had medical insurance cover. A larger proportion 82.6% (n=123) of the respondents had made arrangement on who could make decision in case of an obstetric emergency, of these, 42.3% (n=63) appointed their husbands as the decision maker. Overall, 90.6% (n=135) reported readiness for complications.
|
3.3. Knowledge of Obstetric Danger Signs
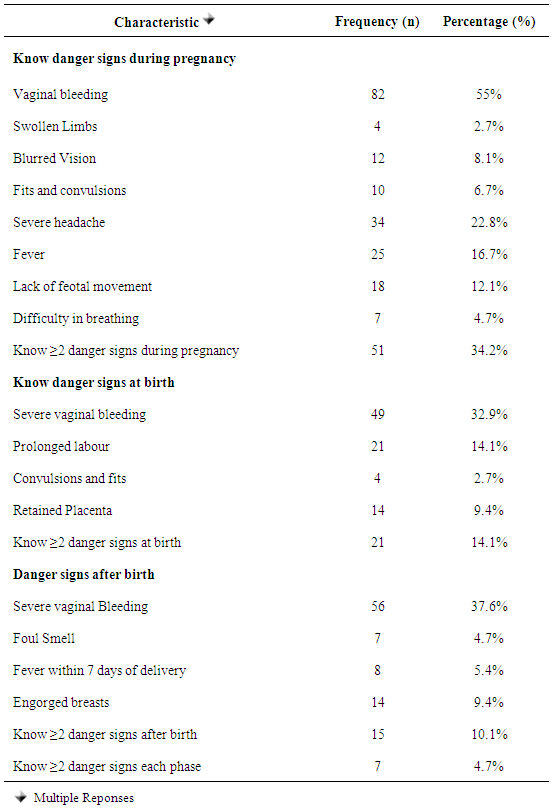
- The most common mentioned danger sign during pregnancy was vaginal bleeding 55% (n=82), severe headache by 22.8% (n=34) and lack of foetal movement by 12.1% (n=18). The least mentioned danger sign during pregnancy was swollen limbs 2.7% (n=4). At birth, the most mentioned danger sign was severe vaginal bleeding 32.9% (n=49). Prolonged labor which is one of the top five major causes of maternal deaths was mentioned 14.1% (n=21). After delivery, severe vaginal bleeding was the most known danger sign by 37.6% (n=56) of the respondents.Overall, 34.2% (n=51) of the respondents were able to mention at least two key danger signs during pregnancy, 14.1% (n=21) during child birth and 10.1% (n=15) during post partum. However, when the scores were combined, only 4.7% (n=7) of the respondents could mention at least 2 key danger signs in all three phases (Table 3).
|
3.4. Factors Associated with Birth Preparedness and Complication Readiness
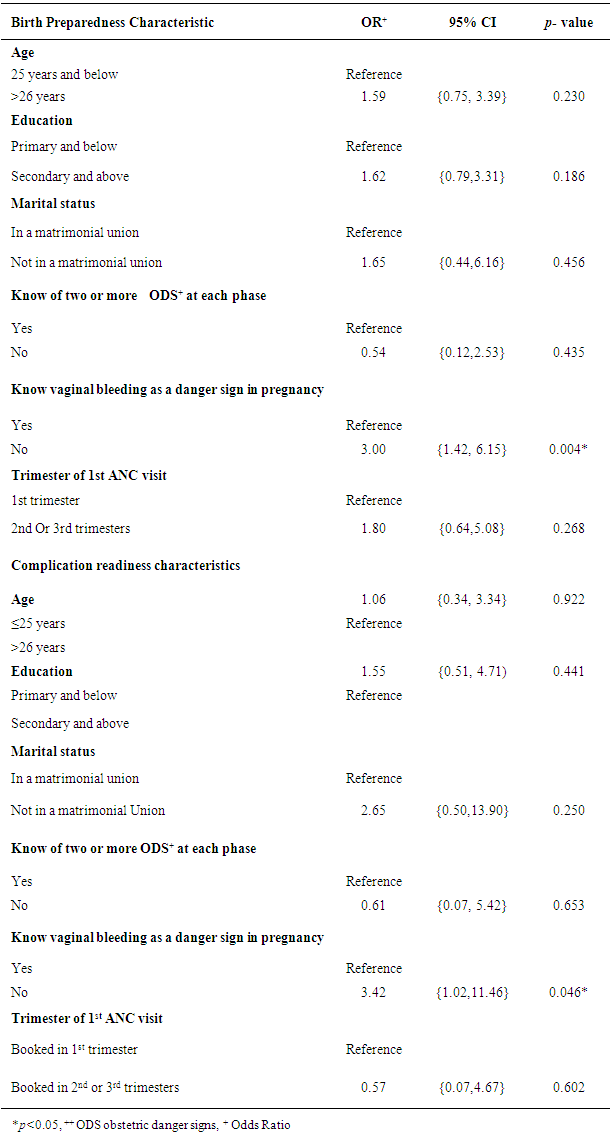
- Table 4 shows the association between demographic factors and both birth preparedness and complication readiness. Women who recognized vaginal bleeding as a danger sign in pregnancy were 3 times more likely to be prepared for birth than those who did not know (OR=3.00, CI 1.43-6.16, p<0.005). Knowledge of vaginal bleeding was also associated with complication readiness (OR=3.47, CI 0.07- 5.42, p<0.005). Demographic variables including age, education, marital status, trimester of first ANC attendance and knowledge of obstetric danger signs were not significant for birth preparedness and complication readiness.
|
4. Discussion
- The study showed that a higher proportion of women reported preparedness for birth and readiness for complications. This proportion is higher compared to previous studies from Uganda [15], Ethiopia [16] and India [17]. The high proportion of birth preparedness and complication readiness reported in the study may be due to the presence of active Community Health Strategy program within the study area and the introduction of free maternal and child health services in all government health facilities. Identification of a place of delivery is a key component of birth preparedness. In the current study, majority of the respondents had identified a place of delivery. Similar result was reported by [8] in Nigeria. However, studies from southern Ethiopia reported that the proportion of women who had identified place of delivery was lower, [16, 18]. Identification of a safe place of delivery is important in reducing the health risks to both the mother and the baby as proper medical attention and hygienic conditions during delivery can reduce the risks of complications and infection that can cause morbidity and mortality to either the mother or the baby. Arranging for transport prior to the date of delivery is essential in reducing the delay in getting to the health facility. In this study, a high proportion of respondents had identified a means of transport to the health facility during delivery and incase of an obstetric emergency. Similar findings were reported from previous studies from Ife, Nigeria [8] and from Kenyatta National hospital, Kenya [14]. However, a lower proportion was reported from Southern Ethiopia [16]. The high proportion that had made arrangements for transport in this study could largely be attributed to the inherent differences in hospital-based and community-based studies. Hospital based studies tend to report high proportions of women having identified a place of birth and arranged for transport compared to community based studies [19].The most common mentioned danger sign during across all phases in this study was vaginal bleeding. This is consistent with studies from Uganda [15] Ethiopia [20] and Tanzania [21]. This is encouraging as27% of all maternal deaths are caused by heamorrhage [22]. This can be attributed to the perceived threat attached to bleeding in all the phases.The proportion of women who knew at least two danger signs at each phase reduces as one approaches post partum. This trend is different in similar studies from Tanzania [23] and Ethiopia [18]. The difference in trend of knowledge of danger signs in the three countries is attributed to the different unique settings among the countries.In the current study, only 4.7% knew at least two danger signs at each phase namely pregnancy, delivery and post-partum. Similarly, studies conducted in Tanzania [23] and Ethiopia [18] have reported low levels of knowledge of at least two danger signs across all the 3 phases. This could be an indication of the missed opportunities during health talks. Most pregnant women come to the antenatal clinics after the health talks have been delivered just to be seen by the nurse to know their progress and go home. Also they may be ignorant of the importance of health educations sessions thus do not make efforts to attend and participate in the sessions.Knowing vaginal bleeding as a danger sign was a strong predictor for birth preparedness and complication readiness in the current study. Women who knew bleeding as a danger sign in pregnancy were 3 times more likely to be prepared for birth and 4 times more likely to be ready for complications compared to those who did not know. Demographic variables including age, education, occupation, marital status, parity, trimester of attendance and knowledge of obstetric danger signs were not associated with both birth preparedness and complication readiness. Therefore, efforts to increase BPCR practices should be targeted at all pregnant women irrespective of their demographic characteristics. The strengths of the study are all the eligible pregnant women who meet the study criteria in the selected health facilities within the period of study were recruited. The study tool was pretested on a similar setting and necessary modifications were made to enhance reliability of the tool. Data collectors were trained and were of the same sex as the respondents. This study had limitations, it was cross sectional hence temporal relationship between variables could not be established. The study targeted women who were attending ante natal care clinic at health facilities hence could have missed views of those who never attend ANC clinics. The findings were self-reported with no means of verification thus subject to bias.
5. Conclusions
- The study showed that a greater proportion of women attending ANC clinic within Bureti Sub County were well prepared for birth and ready for obstetric complications. They also demonstrated adequate knowledge and practice of some of the birth preparedness and emergency readiness. This is a good sign towards reducing mortal mortality. However, the low awareness of obstetric danger signs may be an indication of missed opportunities during health education talks. Low awareness of obstetric danger signs may lead to the first and second delays in seeking health care during obstetric emergencies. Knowledge of vaginal bleeding as a danger sign in pregnancy was a singular predictor for birth preparedness and complication readiness. This is because one will tend to remember what they perceive as a threat. Thus there is need to intensify the health education sessions to all pregnant women irrespective of their demographic characteristics.
ACKNOWLEDGEMENTS
- We also thank to all the pregnant women who honestly gave their responses to make this study a reality.
Funding
- This study was financially supported by National Commission for Science, Technology and Innovation (NACOSTI) -Kenya. The funder had no role in study design, data collection and analysis, or preparation of the manuscript.