Mamedov Umid
Republic Oncology Research Centre, Tashkent, Uzbekistan
Correspondence to: Mamedov Umid , Republic Oncology Research Centre, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Aim: To conduct a comparative analysis of the combined and complex treatment of pharyngeal cancer in combination with surgical method. Material and study methods: 258 patients with pharynx cancer who underwent treatment from 2002 to 2012 have been under our supervision. Results of the study and their discussion: The results of our investigation shows that at the index of T1 in 94.4% cases it was observed full clinical effect. At T2 in 83.6%, T3 in 66.2%, and T4 full effect was registered only in 51% of cases. A partial effect was observed at T2 in 16.4% cases T3 in 22.9%, and T4 in 10.2%. The treatment did not produce positive effect in 11.3%; 26.5%; cases respectively. Conclusions: After treatment and analysis results it has been found that patients with cancer of tonsil gland or base of the tongue tumor had a significantly better clinical outcome of the disease and specific survival was 87.3% (48/55) compared to 67.9% (138/203) of patients with tumors of all other localizations.
Keywords:
Combined treatment, Complex treatment, Brachiotherapy, Pharyngeal cancer
Cite this paper: Mamedov Umid , Combined and Complex Methods of Treatment of Pharyngeal Cancer, American Journal of Medicine and Medical Sciences, Vol. 6 No. 2, 2016, pp. 46-49. doi: 10.5923/j.ajmms.20160602.03.
1. Introduction
Head and neck cancer (HNC) comprises a heterogeneous group of malignancies with a variable clinical course. In the world, HNC is ranked 5th in prevalence, and 7th in mortality [1]. These data are very approximate, since in many countries registration of cancer cases has been poorly organized. There is also a great difference between the regions of the world in the prevalence of head and neck tumors [2]. Although there is a shortage of information on their prevalence in the developing countries, nevertheless, there are still indicators of HNC increase in incidence in many parts of the world caused by the increased consumption of alcohol and tobacco products [3]. One of the most significant prognostic indicators for all localization of squamous cell cancer of the head and neck is the presence of regional metastasis. According to different authors, metastatic affection of regional lymph nodes leads to almost twice reduction in five-year survival and increase in the volume of metastases in the neck progressively reduces life expectancy. Metastatic frequency depends on the organ, where primary tumor is located [4]. Most often, out of head and neck malignancies laryngopharynx cancer metastasizes up to 60% in the primary treatment. With oral mucosa and oropharynx cancer nodal metastases occur in 30-80% of cases [5]. Before the advent of radiotherapy, surgery was the only available treatment for patients with head and neck tumors. After radiotherapy advent it became gradually replaced by surgical treatment [6]. However, at the present moment these two methods of treatment are being used together [7]. Within the last few years, the surgeons have sought to decrease mortality and disability of patients, due to which new treatment techniques have been worked out and improved [8].
2. Aim of the Study
To conduct a comparative analysis of the combined and complex treatment of pharyngeal cancer in combination with surgical method.
3. Materials and Methods
In 258 patients with pharynx cancer who underwent treatment from 2002 to 2012 have been under our supervision.
4. Results of the Study and Discussion
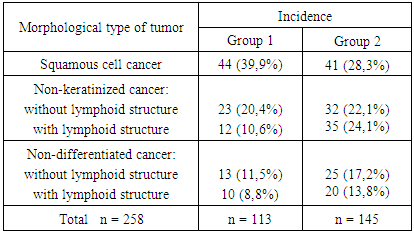
Analysis of the study is based on retrospective and prospective study of treatment results in patients with pharynx cancer. According to the conditions of our study, diagnosis for all patients was confirmed by morphological methods. Table 1 shows that 1/3 of all patients had squamous tumor structure, and more frequently non-keratinized carcinoma (43.4%) was found in patients.Table 1. Morphological structure of nasopharyngeal tumor included into research
 |
| |
|
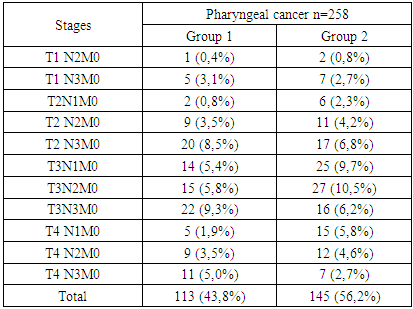
Control over the affected cervical lymph nodes during monitoring was carried out by ultrasound with fine-needle biopsy of suspicious metastatic lymph nodes. For all patients the diagnosis was confirmed by morphological methods. According to the method of treatment patients were divided in the following groups: patients of the Group 1 were administered 2 stages treatment: stage 1- chemo-radiotherapy, stage 2 - surgical treatment (94 patients); Group 2: stage 1 - surgical treatment, stage 2 – chemo-radiotherapy (83 patients); Group 3: stage 1 - radiation therapy, stage 2 - surgical treatment (81 patients) (Table 3). All patients received combined or complex treatment. In some cases (37 patients) of insufficient resorption of nasopharyngeal tumor after 60 Gy external radiotherapy further were given intracavitary therapy (brachytherapy) up to TFD eq. to 80 Gy.Table 2. Disturbances of patients according to stages
 |
| |
|
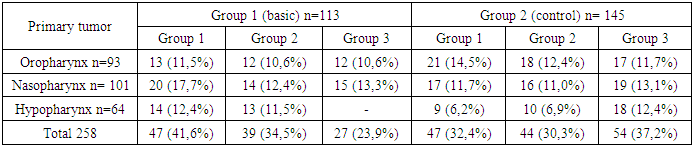
Selection of therapy tactics and priority of conducting special treatment methods depend on the primary tumor origin. In case of oropharyngeal tumors, most of primary tumors are easily removed surgically, as for nasopharynx tumors, due to their clinical and anatomical features it is rather difficult to use surgical method. The following table provides data on localization of the primary tumor and used therapy tactics depending on the study group (Table 4).Table 3. Disturbances of patients with pharyngeal cancer due to study groups
 |
| |
|
Table 4. Disturbances of patients according to primary tumor localization and used therapy tactics
 |
| |
|
In the main group allocation of patients according to the chosen treatment strategy was identical. Patients with Hypopharynx tumors of the main group were treated by various combinations of chemoradiotherapy with surgical therapy, treatment regimens without chemotherapy in these patients have not been provided. With regard our study objective aimed at improvement of surgical treatment results and rehabilitation of patients with oropharyngeal tumors with regional metastases, it was planned to develop a new method of extended lymphadenectomy with resection of the neurovascular neck structures. Next, we decided to consider in more detail the surgical techniques used in this study. In the group of patients, who underwent surgical treatment, after neoadjuvant chemoradiotherapy single-step excision of the primary tumor with lymph node dissection was performed in the main group of 47 patients in 21 (44.7%) cases. From them, in 7 (14.9%) cases it was for oropharynx tumor, in 5 (10.6%) cases for nasopharyngeal tumors, and in 9 (19.1%) cases for hypopharynx cancer. In 26 (55.3%) cases only cervical lymph node dissection was performed. In the control group the similar treatment was provided for 47 patients, from whom in 17 (36.2%) cases was performed single-step removal of the primary tumor and cervical lymph node dissection, and in 30 (63.8%) cases only the dissection of the cervical lymph nodes. Single-stage surgery was performed in the control group of 17 patients in 10 (27.0%) cases for oropharyngeal tumor, in 5 (13.5%) cases for nasopharyngeal tumors, and in 2 (5.4%) cases for hypopharyngeal tumors.In the second study group from 39 patients of the main group in 17 (43.6%) cases was performed single-stage surgery for the primary cancer, and in the area of regional lymph collector, in 22 (56.4%) cases only cervical lymph node dissection. From 17 patients 8 ones (20.5%) were ill with oropharynx cancer, 6 (15.4%) with nasopharynx cancer, and 3 (7.7%) patients with Hypopharynx cancer. In the control group consisting of 44 patients in 11 (25%) cases was performed single-stage surgery, from them 7 (15,9%) for oropharynx tumor, 3 (6,8%) for nasopharynx, and 1 (2,3%) for hypopharynx. In the third group of 27 patients of the main group in 12 (44,4%) cases was performed singe-staged surgery, and in the control group for 19 (35,2%) patients from 54. In other cases, surgical intervention was limited to the dissection of regional lymph nodes. Removal of primary tumor was performed in 9 (30%) for oropharynx cancer, in 3 (11.1%) for nasopharynx. In the control group there were 6 (11.1%) patients with oropharynx cancer, 9 (16.7%) with the nasopharynx and 4 (7.4%) patients with a hypopharynx cancer. Removal of the primary tumor was performed in 117 patients of which 50 (42.7%) patients of the main group and 67 (57.3%) patients of the control group. Various types of regional lymph node dissection were performed in 113 (100%) patients of the main group and 103 (71.0%) patients of the control group.Results of treatment in the main and control groups were the same because of using identical therapeutic regime and strategy. Table 5 shows that full effect was observed in 60% of cases, and almost in a quarter of cases the treatment gave partial effect. In patients with large tumors or massive regional metastases treatment did not always give a positive result, in this study a share of such patients was more than 16%.Table 5. Disturbances of patients according to primary tumor localization and used therapy tactics
 |
| |
|
In the group of patients with partial effect, results of resorption of the primary tumor and regional metastases were different. For example, from 46 patients with partial response to treatment, in 31 (15.6%) cases has been observed full resorption of the primary tumor, but there was no full resorption of metastatic nodes. The reason for this is the use of different doses of the primary focus areas and regional metastasis.In 199 patients was observed an immediate effect of the primary tumor treatment. From them, there were 84 patients of the main group, where the first stage of the lesion treatment (T) was chemoradiotherapy performance. In the control group of patients, in 115 cases the first stage was also chemoradiotherapy performance followed by surgery care (Table 5). The results of our investigation shows that at the index of T1 in 94.4% cases it was observed full clinical effect. At T2 in 83.6%, T3 in 66.2%, and T4 full effect was registered only in 51% of cases. A partial effect was observed at T2 in 16.4% cases T3 in 22.9%, and T4 in 10.2%. The treatment did not produce positive effect in 11.3%; 26.5%; cases respectively. The progression of the process was noted in 8 cases, in two cases the tumor had T3 (4.2%), in six cases at T4 (12.2%). Observed insignificant (F = 0, 17) better results in the main group were associated with the advent of better drugs in the market.
5. Conclusions
1. After treatment and analysis results it has been found that patients with cancer of tonsil gland or base of the tongue tumor had a significantly better clinical outcome of the disease and specific survival was 87.3% (48/55) compared to 67.9% (138/203) of patients with tumors of all other localizations.2. In patients after external beam radiotherapy having viable tumor cells in biopsy materials from cervical lymph nodes mortality prognostics was worse due to disease progression by 52% compared to 10% of patients without viable tumor cells in the neck region.3. Overall survival was 62% and disease - specific survival was 76%. There were no significant differences in disease-specific survival between patients N1 (23.5%, 8/34) and patients with N2-3 (23.8%, 39/164) (p = 0.91). Also, there were no differences between groups of patients when compared only to patients with the full effect (p = 0.95).
References
| [1] | Amiraliev NM, Goldobenko GV, Tkachev, S., et al. Thermoradiotherapy patients with metastatic laryngeal cancer in the lymph nodes in the neck. - Abstracts of the II Congress of CIS Oncologists, Kiev, May 23-26, 2000. - vol. 22. - suppl. 400. |
| [2] | Karasev V.V., Kitsmanyuk Z.D., Musabaeva L.I., et al. Chemoradiotherapy in patients with locally advanced cancer of the oral cavity and oropharynx. - Ros. Oncol. Journal. - 2000. - № 4. - P. 21-23. |
| [3] | Mejidov MG Current approaches to diagnosis and treatment of locally advanced cancer of hypopharynx (T3.4N0-3M0). - Diss .... Dr. ramed. Sciences. - M. - 2005. P. 236p. |
| [4] | Gladilina IA Aliev BM Goldobenko GV Long-term results multifraktsionirovannogo irradiation of oropharyngeal cancer patients III-IV stages of the disease. - Questions of Oncology. - 2000 - 46 m, № 1. P. 44-49. |
| [5] | Gurevich Y.B. Radiotherapy regional metastases of cancer of the larynx and oropharynx as an alternative to surgery. -Avtoref. diss. ... Cand. honey. Sciences. – M.A. – 2002. P. 31. |
| [6] | Amdur R.J., Parsons J.T., Mendenhall W.M. et al. Postoperative irradiation for squamous cell carcinoma of the head and neck: an analysis of treatment results and complications // Int. J. Radiat. Оncol. Вiol. Рhys. – 1989. – Vol. 16. – P.25536. |
| [7] | Borges A.M., Shrikhande S.S., Ganesh B. Surgical pathology of squamous cell carcinoma of the oral cavity. Its impact on management // Semin. surgical oncology. – 1989. – №5. – P.3100317. |
| [8] | Wang Z.H., Million R.R., Mendenhall W.M. et al. Treatment with preoperative irradiation and surgery of squamous cell carcinoma of the head and neck // Cancer (Philad.), 1989. – Vol. 64. – P.32238. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML