-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2016; 6(2): 40-45
doi:10.5923/j.ajmms.20160602.02

Pathogenesis of Vitiligo and Development of Formulation for Its Treatment
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLBotir Saatov 1, Saidkasim Arifov 1, Oibek Umerov 2
1Department of Dermatology, Republican Center of Dermatology and Venereology, Uzbekistan Ministry of Public Health, Tashkent, Republic of Uzbekistan
2Laboratory of Metabolomics, Institute of Bioorganic Chemistry, Uzbekistan Academy of Sciences, Tashkent, Republic of Uzbekistan
Correspondence to: Botir Saatov , Department of Dermatology, Republican Center of Dermatology and Venereology, Uzbekistan Ministry of Public Health, Tashkent, Republic of Uzbekistan.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Key pathogenetic factors of vitiligo, a widely spread skin disease, have been studied. High level of oxidative stress and phospholipid composition disorders in the depigmentated skin area in patients with vitiligo has been established. On the basis of findings, multi-component liposomal formulation intended for pathogenetic therapy of vitiligo has been obtained. Liposomes were constructed from phospholipids and cholesterol isolated and purified from the bovine brain extracts. The liposomal formulation for topical application on the affected skin area of the patients was used in combination with ultraviolet light therapy in treatment of 42 patients with vitiligo. Following three courses of therapy, depigmentation with various degrees of intensity was registered in 97.6% of the patients; in 14 patients (33.3%) total clinical cure was observed. The liposomal formulation demonstrated high efficacy while applied topically in therapy of vitiligo.
Keywords: Catalase, Liposomes, Oxidative stress, Phospholipids, Vitiligo
Cite this paper: Botir Saatov , Saidkasim Arifov , Oibek Umerov , Pathogenesis of Vitiligo and Development of Formulation for Its Treatment, American Journal of Medicine and Medical Sciences, Vol. 6 No. 2, 2016, pp. 40-45. doi: 10.5923/j.ajmms.20160602.02.
Article Outline
1. Introduction
- Vitiligo, also called leukoderma, is an acquired dermatosis of chronic course with typical manifestations in the form of white patches resulting from sharp reduction or absence of melanocytes producing melanin. Vitiligo is a widely spreadhuman disease with mean prevalence in the world population of 1-2% [1-3]. Recently, number of patients with vitiligo has intensively increased, among children, young adults and persons of workable age, in particular, significantly deteriorating their life’s quality and imparting social value to the dermatosis. Nevertheless, pathogenesis of the disorder remains unestablished, and there are no efficient methods to manage the disease. As to pathogenesis of vitiligo, there are several consistent hypotheses, such as, genetic, neuroendocrine and autoimmune ones, as well as a theory of biochemical disorders, and oxidative stress [4, 5, 2, 6]. Significance of oxidative stress for mechanism of vitiligo onset and progression was confirmed by some authors demonstrating imbalance between oxidative effects and anti-oxidant protection of the skin [4, 7-9]. In its turn, oxidative stress results in damage of melanocytes and appearance of the depigmentated skin areas due to excessive accumulation of toxic free radicals [9-11]. Information on positive effect of antioxidants in therapy of vitiligo can serve as an indirect proof of the role oxidative stress plays in pathogenesis of vitiligo [5]. Of note, oxidative stress was proposed as a causative factor in vitiligo pathogenesis while ago [5]. It follows that medical interventions designed for inhibition of oxidative stress can be an efficient approach in therapy of vitiligo.It should be noted that structural-metabolic studies of the skin in vitiligo, in particular, are practically absent. There is no literature data about studies on the human skin phospholipids, structural basis for membranes of pigment cells. It is a destruction of membrane structures of melanocytes under various effects that is considered a key factor of vitiligo’s pathogenesis.Liposomes are nano-vesicles formed from phospholipids and cholesterol under the effect of physical and chemical factors. They serve as a substance for liposomal medications and cosmetics. Liposomes are able to include various agents soluble both in water and in lipids. The delivery of physiologically active substances and medications into a cell is the essential function of liposomes. Extreme durability, flexibility, non-toxicity, biocompatibility and biodegradability are the unique properties of liposomes allowing their wide use in medical and cosmetic formulations [11, 12].Thus, by encapsulation of biologically active substances, vitamins, antioxidants and microelements it is possible to deliver them into the deep layers of the skin, to change metabolic processes, and to improve physiological and pathological conditions of the skin. The work was initiated to study basic links of metabolic disorders in the skin in vitiligo, and to reduce oxidative stress and modify phospholipids composition of the skin in patients with vitiligo by means of a liposomal formulation.
2. Materials and Methods
2.1. Patients
- There were 195 patients with vitiligo, 88 (45.2%) women and 107 (54.8%) men among them, aged from 12 to 55 years with the disease duration from 5 months to 12 years under therapy at the Republican Specialized Research Center of Dermatology and Venereology, Uzbekistan Public Health Ministry.
2.2. Biochemical Investigations
- Biochemical investigations were performed on biopsy material of healthy skin and the depigmentated areas of patients with vitiligo, as well as on the patients’ blood serum samples. Extraction of total lipids from biological objects and their purification from non-lipid impurities was performed by Folch’s method (1957) [13] with recommendations of Kates (1975) [14] with chloroform- methanol mixture (2:1). The purified total lipid extracts of skin and blood serum were used to determine sum of phospholipids and their fraction composition.
2.3. Quantitative Assay of Phospholipids and Their Fractions
- Content of phospholipids and their individual fractions was determined by amount of phosphorous in them after mineralization of total lipid samples and their fractions with subsequent colorimetric assay of the non-organic phosphorus formed [15]. Fraction composition of phospholipids was investigated by thin-layer chromatography on KCK silica gel in the system of solvents (chloroform-methanol-acetic acid-water, 16:4:1:4). Each of the fractions was scraped from the plates which were subjected to mineralization in the presence of the concentrated perchloric acid within aluminum blocks at 200°C. Non-organic phosphorus formed as the result was determined as above by Vaskovsky et al., (1975) [15].
2.4. Determination of Lipid Peroxidation and Activity of Catalase
- Lipid peroxidation in the skin and blood serum was studied by amount of its end product, malondialdehyde (MDA) by means of thiobarbituric acid [16]. Activity of catalase in blood and homogenates of biopsy skin material was measured by intensity of disintegration of H2O2 in the presence of ammonium molybdate [17].
2.5. Preparation of Liposomal Formulation
- Liposomes were produced from phospholipids and cholesterol obtained from the bovine brain. To isolate lipids definite weighted amount of the brain tissues was thoroughly washed from blood by means of cold physiological solution, purified of connective tissue, desiccated and weighted with subsequent homogenization. The homogenate was embathed with chloroform-methanol (2:1, v/v) mixture in an amount 20 ml per 1g of tissue. Extraction was performed within 60 minutes with regular shaking of content of flasks at the room temperature. The method allowed getting almost complete (up to 98%) extraction of tissue lipids. Subsequently, the extract was filtered through glass filters in the vacuum. 0.74% KCl solution was added to the filtrated extract (5:1). Following thorough mixing to separate organic and aqueous-methanol phases, the mixture was centrifuged for 30 minutes at 5,000 rpm. Upper, aqueous-methanol phases including non-lipid additive elements were removed. Lower, chloroform-methanol phase including all tissue lipids was dried lyophilically. Dry residue was embathed with acetone to precipitate phospholipids. Cholesterol from acetone solution was isolated chromatographically to separate cholesterol by a system of solvents consisting of ether- benzol-ethanol-acetic acid (40:50:2.02, v/v). Preparations of phospholipids from the bovine brain and cholesterol were used to prepare liposomes. Liposomes were constructed from phospholipids and cholesterol (7:1) by conventional methods with ultrasound processing. Tyrosine, cupirum (copper preparation), selenium and α-tocopherol were encapsulated into the liposomes. The end product, a liposomal formulation, is a milky, slightly opalescent viscous emulsion. The formulation was approved for topical application in patients with vitiligo by the National Ethical Committee, Uzbekistan Public Health Ministry (Abstract of the minutes No.4 dated April 7, 2010).
3. Results and Discussion
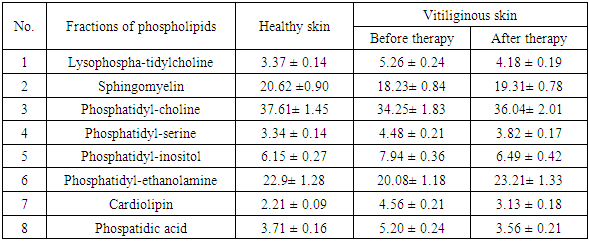
- We compared phospholipid composition in the skin of patients with vitiligo and healthy controls. Significant reduction in the content of total phospholipids in the depigmentated areas of the patients as compared with the similar parameters in healthy subjects was established.Total phospholipids in healthy and the affected skin are 1324.4 ± 57.9 μg and 1157.5 ± 52.8 μg of lipid phosphorus per 1 g of dry tissue, respectively (Table 1). In contrast to the normal skin, increase in the content of lysophosphatidylcholine and phospatidic acid was observed in the depigmentated areas of the patients’ skin. In the skin of patients with vitiligo neutral fractions of phospholipids, such as phosphatidylcholine, phosphatidylethanolamine and sphingomyelin were found significantly reduced. Thus, considerable changes can be seen in the phospholipid composition of the vitiliginous skin.
|
|
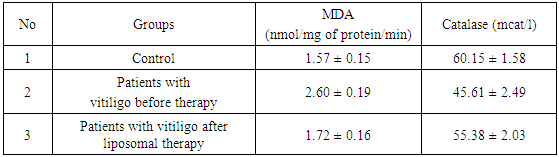
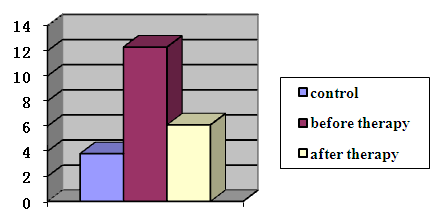 | Figure 1. Content of MDA in the skin of healthy subjects and patients with vitiligo (nmol/mg of protein/min) |
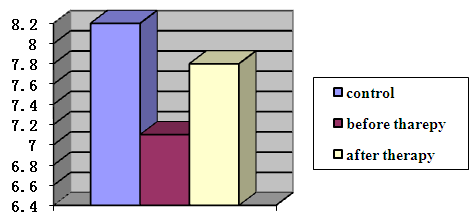 | Figure 2. Catalase activity in the skin of healthy subjects and patients with vitiligo (mcM H2O2/mg of protein/min) |
 | Figure 3. Patient A. with vitiligo (a) before and (b) after liposomal therapy |
 | Images of biopsies (skin bioptate as an object of biochemical investigation) |
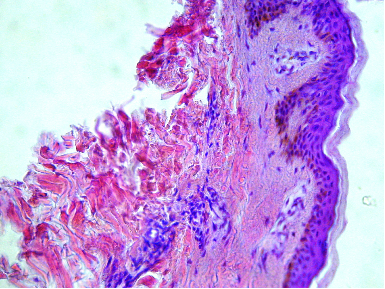 | Non-affected area |
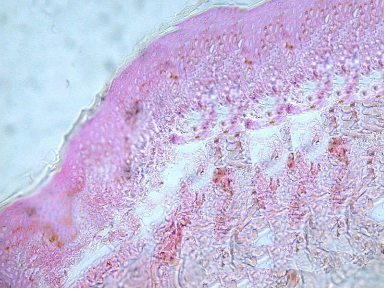 | Affected area |
4. Conclusions
- Fraction composition of the human’s skin phospholipids in healthy subjects and patients with vitiligo was studied. Phospholipid composition of the depigmentated areas in patients with vitiligo was found to significantly differ from the one in healthy subjects. In contrast to healthy subjects, high level of oxidative stress both in the skin and blood of patients with vitiligo was established. Abnormalities in phospholipid composition of the skin and increased intensity of oxidative stress are thought to be essential pathogenetic factors contributing to onset and progression of vitiligo. A multi-component liposomal formulation intended for topical application in pathogenetic therapy of vitiligo has been developed. Topical application of the liposomal formulation demonstrated high efficacy as compared with other methods of treatment of vitiligo; the formulation was recommended for wide use in therapy of the dermatosis.
ACKNOWLEDGMENTS
- The authors are very grateful to Prof. T. Saatov for valuable discussion and suggestions to improve the quality of paper.