Adekunle Olatayo Adeoti, Ebenezer Adekunle Ajayi, Akande Oladimeji Ajayi, Samuel Ayokunle Dada, Joseph Olusesan Fadare, Michael Akolawole, Kehinde Adesola Adekeye, Taiwo Hussein Raimi
Department of Medicine, Ekiti State University Teaching Hospital, Ado-Ekiti, Nigeria
Correspondence to: Adekunle Olatayo Adeoti, Department of Medicine, Ekiti State University Teaching Hospital, Ado-Ekiti, Nigeria.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
Abstract
Background: The trend in medical admission is very dynamic and it is very important for planning, policy formulation and assessment of health status of the populace. Aim: To investigate the pattern and outcome of medical admissions in Ekiti State University Teaching Hospital, Ado-Ekiti, over a period of 5years. Method: Medical records of adult admissions between January 2008 and December 2012 were reviewed for the retrospective study. Results: A total of 3750 patients were admitted with a male to female ratio of 1.1 to 1. The mean age was 50.87±19.82 years and the age range was 16 to 102 years. Non communicable diseases constituted a majority of the admissions with the highest percentages in persons with stroke (21%), diabetes mellitus (18%), systemic hypertension (13%) and heart failure (11%). Notably, communicable diseases (CD) ravaged the young adults where HIV/AIDS (73.0%), pulmonary tuberculosis (60.0%), and malaria (60.0%) affected this age group. Overall mortality rate was 16.0%. Stroke, diabetes mellitus, HIV/AIDS, pulmonary tuberculosis and heart failure accounted for most deaths. Patients with NCD stayed longer on admission than those with CD (8.37±8.07 vs 7.18±7.24 days, p<0.0001), although patients with stroke, diabetes mellitus and HIV/AIDS stayed longest. Conclusions: In view of the huge burden of NCD and CD in the elderly and young adults respectively found in this study, the need for aggressive preventive measures and scaling-up resources for quick intervention to curb this menace is imperative.
Keywords:
Medical admissions, Communicable diseases, Non communicable diseases, Nigeria
Cite this paper: Adekunle Olatayo Adeoti, Ebenezer Adekunle Ajayi, Akande Oladimeji Ajayi, Samuel Ayokunle Dada, Joseph Olusesan Fadare, Michael Akolawole, Kehinde Adesola Adekeye, Taiwo Hussein Raimi, Pattern and Outcome of Medical Admissions in Ekiti State University Teaching Hospital, Ado-Ekiti- A 5 Year Review, American Journal of Medicine and Medical Sciences, Vol. 5 No. 2, 2015, pp. 92-98. doi: 10.5923/j.ajmms.20150502.06.
1. Introduction
Nature of health related conditions across populations and the intriguing imbalance in the rate of reproduction and death has been a subject of discussion since primeval times. [1, 2] Presumably, the prevailing ailments in the society is said to determine the trend in hospital admissions which will also give an overview of the health status of the community. Therefore, hospitalization often gives an idea of the dynamics in disease pattern in a community, although, the precise prevalence of such might not be determined. [3] This insight is important for planning, policy formulation and eventually will determine the allocation of resources for health services, research and training. [4] Information in this regard is often lacking, especially in developing countries, which would have been helpful in the proper distribution of the meager resources allocated to healthcare in such setting. [4] Lately, the drift towards non-communicable diseases (NCD) as the leading cause of medical admission in developing countries due to epidemiological transition have been highlighted, [1, 3, 5, 6] however the communicable diseases (CD) still account for a bulk of patients by virtue of its high burden in the developing countries. [3] Previous studies on the pattern and outcome of medical admission in hospitals in Nigeria [4, 5, 7-9] have been documented but none to the best of our knowledge in Ekiti state, south western, Nigeria. This study aimed at describing the pattern and outcome of medical admissions in a sub-urban tertiary institution in Ekiti state, Nigeria and compared it to previous studies.
2. Methods
This retrospective study was conducted at the Ekiti State University Teaching Hospital (EKSUTH), Ado-Ekiti, Ekiti State, Nigeria between January 2008 and December 2012. All medical admissions during this period were included in the study. EKSUTH is a 300 bed hospital with 46 devoted for admission of adult male (23 beds) and female (23 beds) medical cases. Patients are admitted to the medical ward via accident and emergency unit, medical outpatient and general outpatient clinics. It is located in south western part of Nigeria, serving as a tertiary centre for 16 General Hospitals and 32 Comprehensive health centers in the state that cater for the health needs of a population of over 2 million people. Referrals are also received from neighbouring states of Kwara, Osun, Ondo, and Kogi within the catchment area of 150km radius. Eight Physicians are saddled with the responsibility of determining the final diagnosis of admitted patients and their work is often complemented by the results from the laboratories and radiology units.Admission and discharge records were retrieved and the following information was captured: name, age, hospital number, sex, duration of hospital stay, outcome of treatment. Outcome variables were discharge following improvement, death, referred to other hospitals and left against medical advice. Medical diagnoses of the admitted patients were categorized using ICD-10 coding system. Institutional ethical approval was obtained from the hospital’s ethical committee. The data were analyzed with Statistical Package for Social Sciences (SPSS Inc, Chicago, version 20.0). Continuous variables were expressed as means ± standard deviation while categorical variables as frequencies and percentages. Comparisons of categorical data were performed using Pearson’s chi-square test and p value of less than 0.05 was considered as statistically significant.
3. Results
During the study period of five years (January 2008 to December 2012), a total of 3,750 patients were admitted into the male and female wards which constituted 1963(52.3%) males and 1787(47.3%) females with a male to female ratio of 1.1 to 1. The mean age was 50.87±19.82 years with age range of 16 to 102 years. The male patients were older (51.81±19.82 vs 49.84±19.78 years; p=0.002). About two third of patients admitted were younger than 65 years.
3.1. Pattern of Diseases
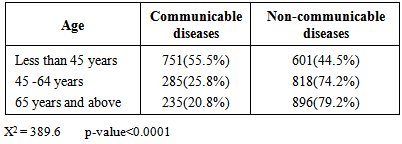
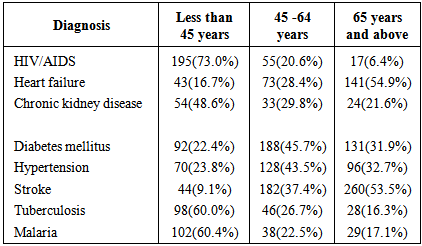
Non-communicable diseases 2315(64.6%) constituted the majority of admitted cases during the period under review [Figure 1]. The major non-communicable diseases (NCD) were stroke (21%), diabetes mellitus (18%), hypertension (13%), and heart failure (11%) while the main cases of communicable diseases (CD) admitted were HIV/AIDS (21%), pulmonary tuberculosis (16%) and malaria (13%). Despite constituting the same percentage in their individual groups, stroke and HIV/AIDS represented 13.6% and 7.4% of the total medical admissions respectively. With increasing age, there was a stepwise rise in the number of NCD admitted whereas a decline with increasing age was observed in the number of patients with CD [Table 1]. As shown in Table 2, the young adult population had more admissions due to HIV/AIDS (73.0%), PTB (60.0%), malaria (60.4%). On the contrary, the elderly patients had a greater proportion of patients admitted with stroke (53.5%), heart failure (54.9%) whereas the middle aged individuals constituted more of those with diabetes mellitus (45.7%), and systemic hypertension (43.5%). Gender distribution of diseases into CD/NCD (figure 2) showed NCD to be more predominant in both sexes and this difference was statistically significant (chi square=7.38, p-Value=0.007).Table 1. Patients’ Age in Relation to Disease Category
 |
| |
|
Table 2. Common Diagnosis in Relation to Patient’ Age Group
 |
| |
|
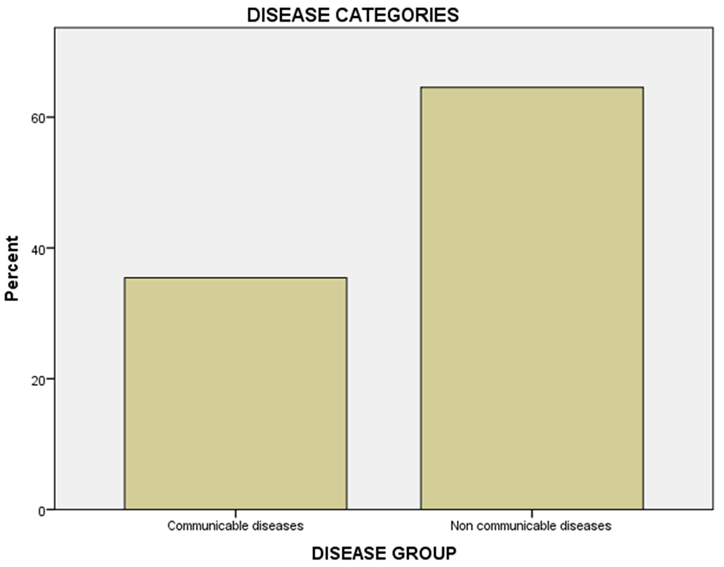 | Figure 1. |
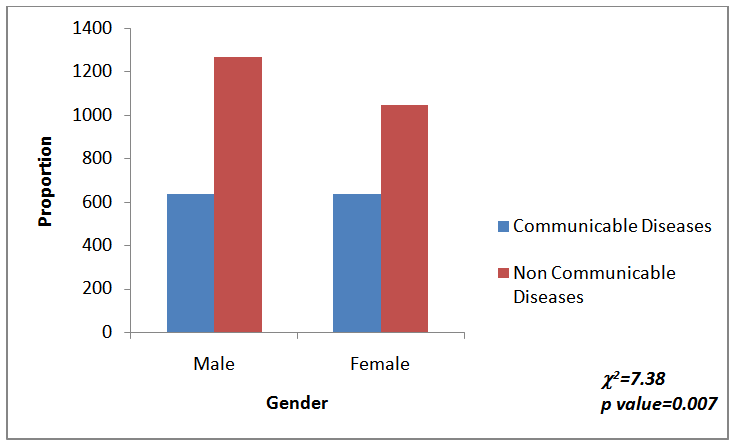 | Figure 2. Gender Distribution of Diseases Categories |
Over the five years period under review, there was a steady decline in admission of both CD and NCD except for a spike in the year 2011(Figure 3).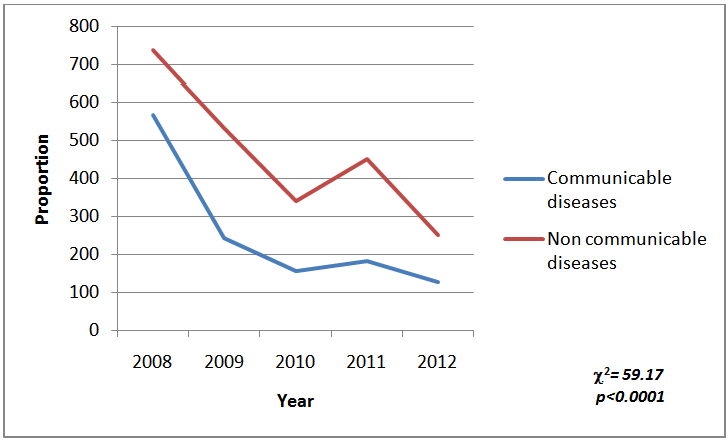 | Figure 3. Trend in Annual Admissions |
3.2. Outcome
A larger percentage of medical admissions (71.1%) were discharged home following remarkable improvement in their clinical conditions. Patients who left against medical advice constituted 7.6%, while those who were referred to other facilities accounted for 5.3% and the mortality was 16.0%. Stroke, diabetes mellitus, HIV/AIDS, pulmonary tuberculosis and heart failure with percentage mortality of 119(21.5%), 64(11.6%), 64(11.6%), 40(7.2%) and 34(6.1%) respectively accounted for most of the cases who died. There was a rise in mortality with increasing age viz 28.7%, 29.6% and 41.6% in the young adults (less than 45years), middle age (between 45 and 64 years) and elderly (65years and above) patients respectively. As shown in figure 4, there was a steady rise in annual mortality rate from the year 2008 to 2011, subsequently a decline in this trend was observed after the year 2011.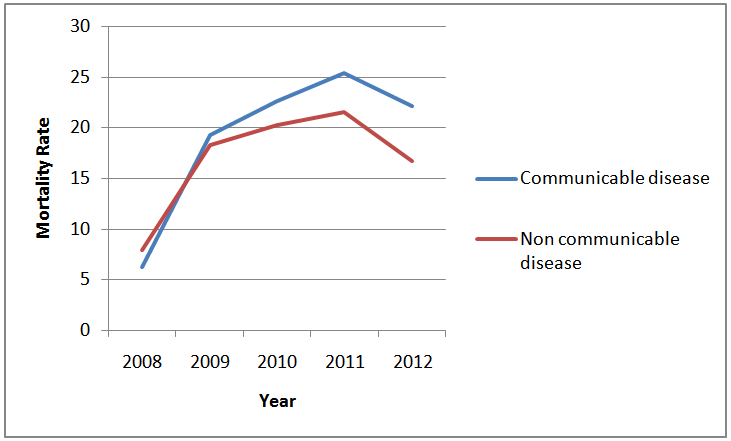 | Figure 4. Trend in Annual Mortality Rate |
3.3. Duration of Hospital Stay
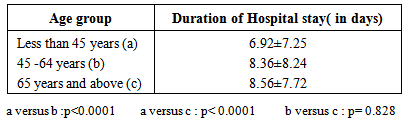
The mean duration of hospital stay was 7.88±7.75 days (range 1-59 days). Males stayed longer than females with a statistically significant difference (8.14±7.98 vs 7.53±7.41 days, p=0.03). The duration of hospital stay increased with patients’ age, as those younger than 45 years had a significantly shorter duration of hospital stay compared to those older than 45 years. The difference in the hospital stay in those between 45 and 64 years and those above 65 years was not statistically significant [Table 3]. Patients with NCD stayed longer in hospital than those with CD (8.37±8.07 vs 7.18±7.24 days, p<0.0001). As shown in Figure 5, based on system involvement, most patients were on admission for the first 20 days however majority of those who stayed beyond 40 days were admitted on account of neurological (mainly stroke) and infectious diseases (mainly HIV/AIDS). The bulk of patients discharged (78.6%) were within the first 20 days likewise those who left against medical advice (75.4%), referred (84.0%) and died (76.3%) as shown in figure 6.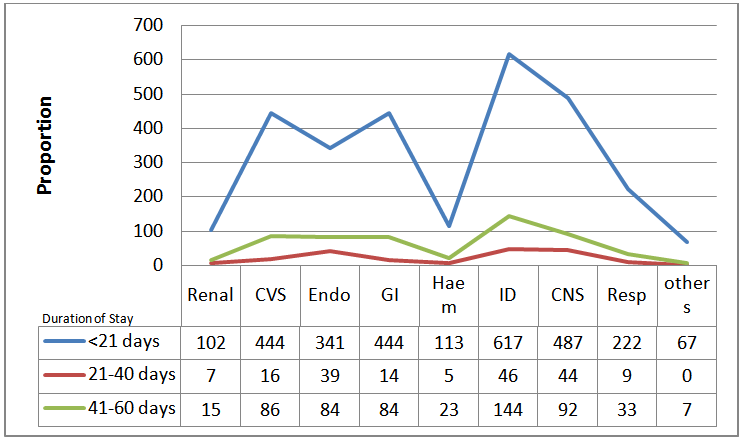 | Figure 5. Duration of Hospital Stay in Relation to Disease Categories |
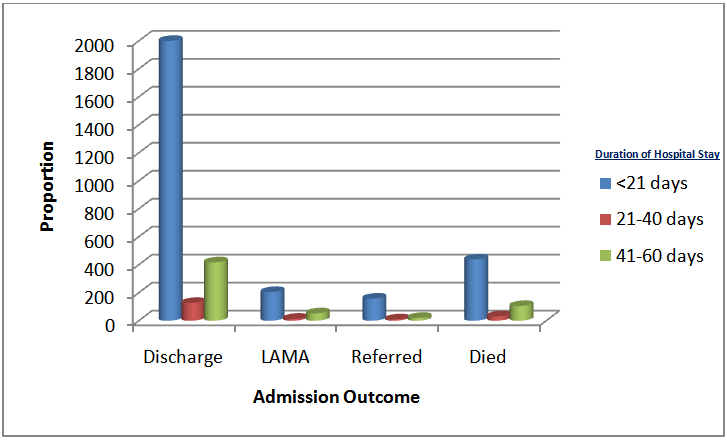 | Figure 6. Duration of Hospital Stay in Relation to Admission Outcome |
Table 3. Patients’ Age Group in Relation to Duration of Hospital Stay
 |
| |
|
4. Discussion
This study has shown a huge burden of both CD and NCD in our locality. However, NCD is a more likely cause of medical admission in EKSUTH, Ekiti State and the elderly patients were more affected. Communicable diseases on the other hand, ravaged the young adults as HIV/AIDS, pulmonary tuberculosis and malaria had higher occurrences in them which could portend an impending epidemic and consequently a huge economic burden.The male preponderance in this study (male to female ratio of 1.1 to 1) is comparable to most similar studies [6, 8, 10] in the country as males being the main earners would likely have more resources to cater for their health needs and would not want to stay out of job for too long hence they would probably attend hospitals earlier than the female counterpart. [11-13] This is however in disagreement with earlier study in Nigeria [4] where female preponderance was found.Similarly, the mean age of patients (50.87±19.82 years) recorded is higher than what was found in the study done by Ogun et al [4] in Nigeria as well as Ali et al [3] in an Ethiopian population but it was comparable to the other findings in Nigeria. [6, 8] Due to control of most childhood killer diseases, more individuals tend to live to adulthood.Contrary to earlier studies where communicable diseases were more prevalent in Nigeria, [4] current research has found a rising trend in admission of patients with NCD. [10, 14-16] This pattern was also seen in our study where NCD accounted for a larger percentage of admissions. This could be explained by the epidemiologic transition in our study population. [2] Stroke was the most common reason for admission and the NCD with the highest occurrence in our study. It was responsible for 13.6% of medical admissions which was higher than 4.5%, 7.3% and 8.7% reported in previous studies in Nigeria. [4, 14, 15] This probably could be due to the rising prevalence of most risk factors for stroke like hypertension and diabetes mellitus in developing countries. [17, 18] Globally, NCD are reaching epidemic proportion and likewise the incidence in the elderly is on the increase. [19, 20] Aging is associated with progressive atherosclerosis and change in circulating hormone concentration which could be responsible for higher occurrence of NCD in the elderly. [21]Unlike other studies where tuberculosis was the commonest CD admitted, [4, 5] HIV/AIDS had the highest percentage among the CD admissions in our study. This high prevalence in our study could be due to ready availability of screening kits and sensitization programmes on HIV/AIDS during which all consenting patients are tested. Tuberculosis, a re-emerging disease, was however second to HIV/AIDS in prevalence among CD which may be fuelled by the interaction between the duo in which HIV/AIDS could cause a reactivation of latent tuberculosis and rapid progression of the disease. [22] Unsurprisingly, young adults were more affected, as they are at the peak of their strength and likely to experiment as well as venture into highly risky behaviours which could expose them to certain communicable diseases.Hospital mortality is a veritable tool for assessing the quality of health care given by an institution. In our study, the mortality rate (16%) was higher than that obtained in western world [23] but similar to findings in some previous studies in Africa. [3, 6, 8] However, it was lower than 23.9% and 25% reported in other parts of Nigeria. [4, 24] The difference may be due to the availability of modern equipment for diagnosis and the presence of more specialists to cater for the patients. Admissions from both NCD and CD accounted for a high disease-specific mortality rate. Patients with stroke had the highest mortality (21.5%) which is comparable to 22.3% reported in south eastern part of Nigeria. [6] Stroke is a major cause of mortality in low and middle income, and the rising prevalence of hypertension and diabetes mellitus often diagnosed when patients would have developed complications. [16, 25] HIV/AIDS and tuberculosis contributed significantly to mortality due to communicable diseases which is in accordance with other studies conducted in Nigeria. [24, 26] The re-emergence of tuberculosis has been attributed to the HIV/AIDS epidemics with a high prevalence in sub-Saharan Africa. Although the prevalence of HIV/AIDS and tuberculosis in Ekiti state is among the lowest in Nigeria, our institution is a major treatment center in our locality and may probably have contributed to the high mortality.Duration of hospital stay was longest in patients with neurological disease (mainly stroke) and infectious diseases (mainly HIV/AIDS). These diseases are associated with severe disabilities and accompanying complications which often warrant longer hospital stay than the other medical admissions resulting in neglect by relatives and sometimes inability to settle hospital bills. [27-29]This study is not without some limitations, one of which is the reliance on the accuracy of the health record for patients’ information as it a retrospective study. In conclusion, with this dual burden of NCD and CD in our study, it is imperative to scale up on preventive measure towards health education and promotion. Furthermore, a boost in healthcare finance, upgrade of health centers as well as training and retraining of staff cannot be over-emphasized.
References
| [1] | Caldwell JC. Population health in transition. Bulletin of the World Health Organization 2001;79(2):159-60. |
| [2] | Cappuccio FP. Commentary: Epidemiology transition, migration, and cardiovascular disease. International Journal of Epidemiology. 2004;33:387-8. |
| [3] | Ali E, Woldie M. Reasons and outcomes of admissions to the medical wards of jimma university specialized hospital, southwest ethiopia. Ethiop J Health Sci. 2010 Jul;20(2): 113-20. |
| [4] | Ogun SA, Adelowo OO, Familoni OB, Jaiyesimi AEA, Fakoya FAO. Pattern and outcome of medical admissions at the Ogun state university teaching hospital, Sagamu- A three year review. West African Journal of Medicine. 2000; 19(4):304-8. |
| [5] | Okunola OO, Akintunde AA, Akinwusi PO. Some emerging issues in medical admission pattern in the tropics. Niger J Clin Pract 2012;15:51-4. |
| [6] | Ezeala-Adikaibe B, Aneke E, Orjioke C, Ezeala-Adikaibe N, Mbadiwe N, Chime P, et al. Pattern of Medical Admissions at Enugu State University of Science and Technology Teaching Hospital: A 5 Year Review. Ann Med Health Sci Res. 2014 May-Jun;4(3):426-31. |
| [7] | Ike SO. The pattern of admissions into the medical wards of the University of Nigeria Teaching Hospital, Enugu (2). Niger J Clin Pract. 2008 Sep;11(3):185-92. |
| [8] | Odenigbo CU, Oguejiofor OC. Pattern of medical admissions at the Federal Medical Centre, Asaba-a two year review. Niger J Clin Pract. 2009 Dec;12(4):395-7. |
| [9] | Etyang AO, Scott JA. Medical causes of admissions to hospital among adults in Africa: a systematic review. Glob Health Action. 2013;6:1-14. |
| [10] | Ogah OS, Akinyemi RO, Adesemowo A, Ogbodo EI. A Two -Year review of medical admissions at the emergency unit of a Nigerian tertiary health facility. Afr J Biomed Res 2012;15:59-63. |
| [11] | Hundley G. Why women earn less than men in self-employment. Journal of Labor Research. 2001; 22(4): 817-29. |
| [12] | Mitra A. Access to supervisory jobs and the gender wage gap among professionals. Journal of Economic Issues. 2003:1023-44. |
| [13] | Okpara JO. Gender and the relationship between perceived fairness in pay, promotion, and job satisfaction in a sub-Saharan African economy. Women in Management Review. 2006;21(3):224-40. |
| [14] | Desalu OO, Wahab KW, Fawale B, Olarenwaju TO, Busari OA, Adekoya AO, et al. A review of stroke admissions at a tertiary hospital in rural Southwestern Nigeria. Annals of African Medicine. 2011;10(2). |
| [15] | Abubakar SA, Sabir AA. Profile of stroke patients seen in a tertiary health care center in Nigeria. Annals of Nigerian Medicine. 2013;7(2):55. |
| [16] | Ajayi EA, Ajayi OA, Adeoti OA, Raimi TH, Fadare JO, Dada SA, et al. A five-year review of the pattern and outcome of cardiovascular diseases admissions at the Ekiti State University Teaching Hospital, Ado Ekiti, Nigeria. Nigerian Journal of Cardiology. 2014;11(1):33. |
| [17] | Ogah OS, Okpechi I, Chukwuonye, II, Akinyemi JO, Onwubere BJC, Falase AO, et al. Blood pressure, prevalence of hypertension and hypertension related complications in Nigerian Africans: A review. World J Cardiol. 2012 Dec 26;4(12):327-40. |
| [18] | Olokoba AB, Obateru OA, Olokoba LB. Type 2 diabetes mellitus: a review of current trends. Oman Med J. 2012;27(4):269-73. |
| [19] | Daar AS, Singer PA, Leah Persad D, Pramming SK, Matthews DR, Beaglehole R, et al. Grand challenges in chronic non-communicable diseases. Nature. [10.1038/ 450494a]. 2007;450(7169):494-6. |
| [20] | Osuji CU, Onwubuya EI, Ahaneku GI, Omejua EG. Pattern of cardiovascular admissions at Nnamdi Azikiwe University Teaching Hospital Nnewi, South East Nigeria. Pan Afr Med J. 2014;17. |
| [21] | Van den Beld AW, Bots ML, Janssen JAMLL, Pols HAP, Lamberts SWJ, Grobbee DE. Endogenous Hormones and Carotid Atherosclerosis in Elderly Men. American Journal of Epidemiology. 2003 157(1):25-31. |
| [22] | Corbett EL, Watt CJ, Walker N, et al. The growing burden of tuberculosis: Global trends and interactions with the hiv epidemic. Archives of Internal Medicine. 2003;163(9): 1009-21. |
| [23] | Papadopoulos IN, Papaefthymiou M, Roumeliotis L, Panagopoulos VG, Stefanidou A, Kostaki A. Status and perspectives of hospital mortality in a public urban Hellenic hospital, based on a five-year review. BMC Public Health. 2008;8(1):28. |
| [24] | Chijioke A, Kolo P. Mortality pattern at the adult medical wards of a teaching hospital in sub-Saharan Africa. Int J Trop Med. 2009;4(1):27-31. |
| [25] | Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJ. Global and regional burden of disease and risk factors, 2001: systematic analysis of population health data. The Lancet. 2006;367(9524):1747-57. |
| [26] | Agomuoh D, Unachukwu C. The Pattern and distribution of communicable diseases among medical admissions in Port Harcourt, Nigeria. Port Harcourt Medical Journal. 2007;1(1): 52-5. |
| [27] | Ajayi E, Ajayi A. Pattern and outcome of diabetic admissions at a federal medical center: A 5-year review. Annals of African Medicine. 2009;8(4). |
| [28] | Bonuck KA, Arno PS. Social and medical factors affecting hospital discharge of persons with HIV/AIDS. J Community Health. 1997 Aug;22(4):225-32. |
| [29] | Van Straten A, Van der Meulen J, Van den Bos G, Limburg M. Length of hospital stay and discharge delays in stroke patients. Stroke. 1997;28(1):137-40. |
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML