-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2015; 5(2): 87-91
doi:10.5923/j.ajmms.20150502.05
Prevalence of HIV-1 and HIV-2 Antibodies in a Cohort of Young Adults Attending Braitwhyte Memorial Specialist Hospital (BMH), Port Harcourt, Nigeria
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLOkonko IO, Nnodim LC
Medical Microbiology Unit, Department of Microbiology, University of Port Harcourt, Port Harcourt, Nigeria
Correspondence to: Okonko IO, Medical Microbiology Unit, Department of Microbiology, University of Port Harcourt, Port Harcourt, Nigeria.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
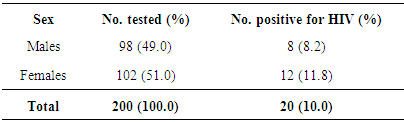
HIV/AIDS is a major public health problem in Nigeria. Thus, this study was carried out to determine the prevalence of HIV-1 and HIV-2 antibodies in a cohort of young adults, ages 16-40 years in Braitwhyte Memorial Specialist Hospital (BMSH), Port Harcourt, Rivers State, Nigeria. Two hundred young adults attending BMH were recruited for this study. There were 102 (51.0%) females and 98(49.0%) males and 109 (54.5%) were within age group 16-30 years of age while 91(45.5%) were within age group 31-40 years old. DETERMINE® HIV-1/2 and HIV-1/2 STAT-PAK® ELISA based kits, were used to detect the presence of HIV-1 and HIV-2 antibodies according to the manufacturer’s specifications. Of the 200 young adults studied, 20 (10.0%) were positive for HIV antibodies. The study showed no significant age (11.0 vs. 8.8, P>0.05) and sex differences (11.8 vs. 8.2, P>0.05) in HIV prevalence of young adults. The 10.0% prevalence of HIV among the young adults studied could be very significant. Although the risk factors (age and sex) analysed were not statistically significant to HIV prevalence as shown in this study, however, public health education is highly needed to highlight the dangers of HIV. In conclusion, this study has further confirmed the presence of HIV-1 and HIV-2 antibodies in a cohort of young adults in Port Harcourt, Rivers State, Nigeria. Early diagnosis of HIV may lead to prompt intervention management towards reducing the vertical transmission of the infection.
Keywords: HIV, Cohort, Antibodies, Prevalence rate, High risk factors
Cite this paper: Okonko IO, Nnodim LC, Prevalence of HIV-1 and HIV-2 Antibodies in a Cohort of Young Adults Attending Braitwhyte Memorial Specialist Hospital (BMH), Port Harcourt, Nigeria, American Journal of Medicine and Medical Sciences, Vol. 5 No. 2, 2015, pp. 87-91. doi: 10.5923/j.ajmms.20150502.05.
1. Introduction
- HIV/AIDS is a major public health problem in Nigeria. HIV belongs to the family Retroviridae, sub-family Ortho-retrovirinae, genus Lentivirus and two species have been identified: HIV-1 and HIV-2 [1, 2]. The pandemic is dominated by HIV-1, which was discovered in 1983 [3, 4]. HIV-1 has been responsible for most HIV infections in the world and HIV-2 is primarily responsible in West Africa countries [1]. In 1987, HIV-2 was discovered which is very common in West Africa1 and has not shown any significant spread from there [3, 4]. HIV-2 is less easily transmitted than HIV-1 and the period between initial infection and illness is longer than with HIV-1 [3-5].Nigeria has the largest population in Africa with a population of over 150 million and HIV prevalence of 4.6% in 2008 [6, 7]. As of 2008, 2.95 million individuals lived with HIV and AIDS in Nigeria and integrated control efforts are immeasurably needed [7-9]. There is therefore, great concern about the spread of HIV epidemic in or within the adolescent population [4, 10]. Over the past years, young adults accounted for 60% of people living with HIV and AIDS, however, 40% of new HIV cases are reported in Africa [4, 11-14]. Most of the new HIV/AIDS infections are heavily concentrated among young people aged between 15-24 years i.e., youths [4, 14]. Thus, this study aimed at determining the prevalence of HIV-1 and HIV-2 antibodies in a cohort of young adults, ages 16-40 years in Braitwhyte Memorial Specialist Hospital (BMSH), Port Harcourt, Rivers State, Nigeria.
2. Methods
- Study designThis was a cross-sectional, consecutive health-facility-based study. In order to obtain a study sample representative of the state, participants were selected from both males and females (ages 16 to 40 years old) attending the attending Braitwhyte Memorial Specialist Hospital (BMSH), in Port Harcourt, Nigeria. To further buttress this, it is a mostly utilized hospital in Rivers State, Nigeria. Ethical considerationsEthical approval was also given by the Rivers State Hospital Management Board. Designated hospital staff members clearly explained, in English or in the individual’s dialect, the objectives and procedures of the study to each prospective participant. Written or oral informed consent was taken from the subjects before enrolment into the study. The participants were assigned identification numbers and were assured that all information obtained would be treated with the utmost confidentiality and used solely for the purpose of this research. Patient Eligibility and Inclusion criteriaApparently-healthy individuals who consented to participate were consecutively recruited for the study. Out-patients 16-40 years of age present at the participating hospital who voluntarily provided informed consent/assent to participate in the study were eligible. All those unwilling to provide informed consent/assent for participating in the study and those aged below 15 years were not eligible. The study was carried out according to ethical research standards. Study populationTwo hundred young adults attending Braitwhyte Memorial Specialist Hospital (BMSH), in Port Harcourt, Nigeria ages 16 – 40 years were recruited for this study. This population was chosen to explore among younger population as a new angle to dissect HIV infection in Nigeria. Accessibility was also another factor for chosen this population. Sexual activities and environmental factors were also another reason for chosen this population. Port Harcourt has a relatively high socio-economic status and the people are predominantly Ibos, Ikwerre, Okirika, Ogoni, with other tribes from various parts of the country and outside Nigeria. Braitwhyte Memorial Specialist Hospital (BMSH) is one of the specialist hospitals in Port Harcourt close to Government house and secretariat, which by virtue of its location provides secondary and tertiary health-care services to Old GRA areas and Port Harcourt City, Asari-Tolu, Obio/Akpor, Eleme, Oyigbo and Okirika Local Government Areas in Rivers State, Nigeria.Sample size determinationThe formula n=Z2PQ/d2 was used to derive the desired sample size. Where n is the desired sample size, P is the expected prevalence in the target population, Q is 1-P, Z is 1.96; standard error, d is the level of statistical significance (0.05). A P-value of 7.3% was used representing maximum uncertainty for Rivers State during the last National HIV sentinel study in 2010 [15, 16]. Hence, the estimated sample size was 104 with an additional 10.0% sampled to take care of data inconsistencies [17], providing a total sample size of 115 which was approximated to 200. Thus, N= 200 participants were recruited for this study. Sample collection and plasma preparationSamples were collected in EDTA bottles and carried to the Medical Microbiology Laboratory, Department of Microbiology, University of Port Harcourt, Port Harcourt, Nigeria for analysis using standard laboratory procedures. Blood samples were aseptically collected by venipuncture. A 5-mL blood sample was collected using a disposable sterile needle and syringe from each participant. The blood sample was transferred into a labeled blood sample tube containing EDTA anticoagulant. Plasma was prepared from the clotted blood and stored at – 20℃ until used for serology. Pertinent demographic and behavioral data that might influence transmission and acquisition of HIV were obtained using interviewer-administered questionnaires. Serological TestingAll the consented young adults were screened for antibodies to HIV-1 & -2 using two enzyme-linked immunosorbent assay (ELISA) rapid screening kits, based on World Health Organization (WHO) systems-2 for detecting antibodies to HIV-1 & 2. DETERMINE® HIV-1/2 test kits (Abbott laboratories) were used to screen all samples. Non-Reactive specimens were reported as NEGATIVE. All REACTIVE specimens were confirmed using HIV-1/2 STAT-PAK® (Chembio Diagnostic Systems, Inc.)’ test kits. These kits were designed primarily to test for the presence of HIV-1 and/or HIV-2 antibodies in the blood. Specimens which were positive with both DETERMINE and STAT-PAK test kits were reported as POSITIVE. Specimens which were positive with DETERMINE test kits and negative with STAT-PAK test kits were reported as DISCORDANT. All tests were carried out according to the manufacturer’s specifications. These ELISA based kits are both sensitive and specific (99-100%).Data analysisThe prevalence for HIV-1 and HIV-2 antibodies was calculated by using young adults with positive samples as numerator and the total numbers of young adults enrolled in this study were the denominator. The generated data were presented in descriptive statistics. The data generated were further subjected to Fisher’s Exact Test for comparison of proportions to determine any significant relationship between infection rate and demographical characteristics of the subjects.
3. Results
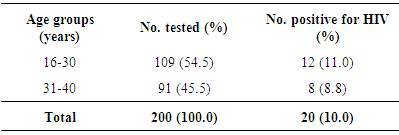
- Of the 200 blood samples analyzed, HIV antibodies were present in 20, giving rise to an overall prevalence of 10.0% for HIV. There were 102 (51.0%) females and 98(49.0%) males. One hundred and nine (54.5%) young adults were within age group 16-30 years of age while 91(45.5%) were within age group 31-40 years old. The study showed no significant age differences (11.0 vs. 8.8, P>0.05) in HIV prevalence of young adults. Age group 16 – 30 years had 12(11.0%) positive samples out of 109 samples analyzed while 8(8.8%) samples in age group 31-40 years were positive for HIV [Table 1].
|
|
4. Discussion
- Young people are central to any discussion about sexuality and acquired immunodeficiency syndrome (AIDS) all over the world [4, 10, 18]. Young people are particularly vulnerable to HIV infection because of the physical, psychological, social and economic attributes of adolescence [4, 19-20]. A more serious challenge today, is the growing infection rates among the adolescents in sub-Saharan Africa [4, 20]. Research has shown that the highest group found to be infected with the virus is the age group 15 to 24 [4, 20-21]. This present study determined the prevalence of HIV-1 and HIV-2 antibodies in a cohort of young adults (ages 16-40 years) in Braitwhyte Memorial Specialist Hospital (BMSH), Port Harcourt, Rivers State, Nigeria. The chosen age group covered and went beyond the much studied age group (15-24 years) as a new angle to dissect HIV infection in Nigeria. From the result obtained, there was an overall prevalence of 10.0% for HIV and it should be noted with astuteness that the kits used were not confirmatory. However, this figure is comparable to the 11.0% reported previously among undergraduate students [22] and the 9.0% reported among street-involved youths in Oyigbo local government area of Rivers State, Nigeria [4]. This prevalence of 10.0% for HIV in this study is higher than the 4.0% reported by Mutinta and Govender [23] among students. It is also higher than the 0.9% reported by Mbakwem-Aniebo et al. [24] among fresh university students. It is higher than the 2.0% reported in our previous studies among secondary school students in Port Harcourt, Nigeria [25] and the 5.5% reported by by Holm-Hansen et al. [26] among students in Tanzania. It is higher than the 4.8% reported by Nwachukwu and Orji [27] among fresh graduates in Nigeria. It is also higher than the 1.0% reported by Holm-Hansen et al. [26] among students at the rural schools in Tanzania. However, 10.0% reported in this study is lower than the 34.29% reported by Akinjogunla et al. [28] in Uyo metropolis. This study found no significant age differences (11.0 vs. 8.8, P>0.05) in HIV prevalence of young adults in Port Harcourt, Nigeria. This might be attributed to their sexual behaviors [4, 23, 29-30]. The present finding of no age associated HIV prevalence is disagrees with the findings of previous studies in some parts of Nigeria and outside Nigeria. In our previous study, a higher prevalence of HIV was reported among youths within age group 21-28 years of age [4]. It deviates from the finding of Mbakwem-Aniebo et al. [24] who reported higher HIV prevalence among age group 20-25years. It deviates from that of Laah and Ayiwulu [31] who reported higher seroprevalence of HIV in age group 20-34 years. Middelkoop et al. [32] showed a high force of infection among adolescents, which positively associated with increasing age. Also, our previous study reported a significant correlation (p<0.05) between the age groups and the prevalence of HIV among undergraduate students ages 20-35 years old in Port Harcourt, Nigeria [25]. The study found no significant sex differences (11.8 vs. 8.2, P>0.05) in HIV prevalence of young adults. This deviated from our previous study [4], where HIV antibodies were more prevalent among female youths in Oyigbo, Rivers State, Nigeria. It also disagrees with our previous study among secondary school students in Port Harcourt, Nigeria [25]. Azuonwu et al. [33] observed a higher female gender predisposition to HIV infection. The present finding also disagrees with the study of Laah and Ayiwulu [31] who reported higher seroprevalence of HIV in females in Nasarawa State, Nigeria. A few studies documented higher prevalence of HIV among males [34].However, this present finding agrees favourably with the findings of some studies in Nigeria. Frank-Peterside et al. [22] reported no significant association with the sex of undergraduate students in Port Harcourt, Nigeria. Mbakwem-Aniebo et al. [24] also reported no significant association with the sex of subjects. This is in agreement with what was reported by Frank-Peterside et al. [35] who showed that females are more prone to HIV and UTI than males. Akinjogunla et al. [28] reported higher prevalence of HIV among females (21.5%) compared to males (12.7%) in Uyo metropolis. Akinjogunla et al [28] suggested that, the high prevalence of HIV among females could be due to prevailing socio-cultural economic scenario.
5. Conclusions
- The 10.0% prevalence of HIV among the young adults studied could be very significant. High occurrence of divorce among young couples could be the cause of high prevalence among young adults. Although the risk factors (age and sex) analysed were not statistically significant to HIV prevalence as shown by the findings of this study. Thus, more public health enlightenment campaign is highly needed to highlight the dangers of HIV. Early diagnosis of HIV may lead to prompt intervention management towards reducing the vertical transmission of the infection. In conclusion, this study has further confirmed the presence of HIV-1 and HIV-2 antibodies in a cohort of young adults in Port Harcourt, Nigeria.