-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2015; 5(1): 26-30
doi:10.5923/j.ajmms.20150501.06
Retrospective Review of Intra Abdominal Injuries Sustained in a Tertiary Teaching Hospital
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAzhar Amir Hamzah 1, Abdul Ghafur Mubarak 1, Rashidi Ahmad 2, Abdul Kareem 3, Amer Hayat Khan 4, Raja Ahsan Aftab 4
1Department of Surgery, Hospital Universiti Sains Malaysia, Kubang Kerian, Malaysia
2Department of Emergency Medicine, Hospital Universiti Sains Malaysia, Kubang Kerian, Malaysia
3Deparment of Radiology, Hospital Universiti Sains Malaysia, Kubang Kerian, Malaysia
4Department of Clinical Pharmacy, School of Pharmaceutical Sciences, Universiti Sains Malaysia, Penang, Malaysia
Correspondence to: Azhar Amir Hamzah , Department of Surgery, Hospital Universiti Sains Malaysia, Kubang Kerian, Malaysia.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
Objective: The aim of this study was to examine patients’ profile and investigation between operatively and conservatively management. Methods: Retrospective record review was conducted. The study identified 86 patients from May 2005 until December 2010 but managed to trace 82 folders. All intra-abdominal injury data were retrieved from medical record. Demographic and in-hospital data were collected. Patients presented to casualty department Hospital USM either from district hospital or direct admission or post motor vehicle accident (MVA) and had an ultrasound or CT scan performed at least by radiology medical officer on admission were included in current study. Results: Fifty five (67.07%) patients were on operative management while 27 (32.93%) were on conservatively management. The common organ detected using CT scan on the patient were bowel (23%) injury followed by liver injury (21%) and splenic injury (19%). None of the patients had gone home and died without apparent cause (from the ones that study managed to contact). Patients died from conservative and operative were 19 and 32 respectively. Study only managed to contact 51 patients (19 from the conservative and 32 from operative group) to assess their quality of life. Operative group return to work less than two weeks was for 32 patients namely 14 patients did not return to work in less than two weeks and among them six had applied for permanent disability. Conclusions: Choosing between operative or conservative management for intra-abdominal injury is crucial part to improve the treatment outcome. Ultrasonography or CT scan were used to identify injuries that can be managed conservatively and rule out others injuries that need surgical treatment.
Keywords: Intra-abdominal, Injury, Conservative management, Operative management
Cite this paper: Azhar Amir Hamzah , Abdul Ghafur Mubarak , Rashidi Ahmad , Abdul Kareem , Amer Hayat Khan , Raja Ahsan Aftab , Retrospective Review of Intra Abdominal Injuries Sustained in a Tertiary Teaching Hospital, American Journal of Medicine and Medical Sciences, Vol. 5 No. 1, 2015, pp. 26-30. doi: 10.5923/j.ajmms.20150501.06.
1. Introduction
- Injury to the abdomen can be difficult condition to evaluate in the hospital setting. Intra-abdominal injury is one of the major causes of preventable traumatic death, the possibility of intra-abdominal injury must be recognized, addressed and documented immediately. Penetrating abdominal injury usually need immediate surgical attention. Blunt injuries (contact sport, motor vehicle collisions, and assaults) may be more subtle, but potentially just as deadly.Understanding the mechanisms of injury is crucial in the management of a patient with abdominal trauma. Apart from various abdominal organs, injury to other parts of body also plays part in ultimate outcome of patient. Many a time minor injury can be serious solid organ damage from into abdominally, such cases should be thoroughly evaluated and managed accordingly.Injuries to the abdomen are usually categorized as blunt of penetrating trauma, but a combination of the two also may occur. It also may involve damage to the abdominal organs. Blunt trauma is the most common mechanism of abdominal injury and has relatively high mortality rates of 10% to 30%. The reason for this is likely related to the frequency of accompanying injury to the head, chest, pelvis, and an extremity in as many 70% of motor-vehicle collision victims.Blunt abdominal injury may be from direct compression of the abdomen against a fixed object with resulting tears or subcapsular hematomas involving the solid organ’s associated viscera (spleen/liver).Computed tomography (CT) scan allows physian to use less surgery because they can identify injuries that can be managed conservatively and rule out others injuries that need surgical treatment.Conservatively management based on CT scan diagnosis and the hemodynamic stability of the patient are now being used in adult for the treatment of solid organ injuries. Advantages of this management include reduced operative complication, reduced transfusion, lower infectious morbidity and shorter length of stay [1]. Multiple studies show than conservatively management of solid organ injuries is a standard care in hemodynamically stable patients with a success rate more than 80% [1-5]. Operative management occurs in hemodynamically unstable patients with hepatic and splenic injuries. It is necessary for patient with penetrating injuries and sign of peritonitis or shock.This study examined the incidence rate involvement of various solid organs, modes of management and outcome of conservative and surgical management in term of mortality rate and quality of life.
2. Methodology
- Retrospective record review was done. All intra-abdominal injury data were retrieved from medical record. Demographic and in-hospital data were collected. Patients presented to casualty department Hospital USM either from district hospital or direct admission or post motor vehicle accident (MVA) and had an ultrasonography or CT scan performed at least by radiology medical officer on admission were included in this study. Patients were excluded if admission with concomitant thoracic or intracranial injuries and only done focused assessment sonography trauma (FAST) scan and managed as per FAST scan (conservative arm). Patient that were included into study were identified and bed history tickets were traced from the record office Hospital USM. The study identified 86 patients from May 2005 until December 2010 but managed to trace 82 tickets. No sampling method was applicable. Patient medical records were retrieved. Patient’s identification, clinical findings, diagnostic test, operative finding and blood tests were extracted using case report form.Conservative management consisted of bed rest, analgesia, hydration and antibiotics in the presence of a urine leak. Patients treated conservatively were routinely reimaged within 48 to 72 hours to enable early detection of complications. Elective retrograde stent placement was considered for persistent, large urine leaks on early repeat imaging in 2 cases. Follow-up imaging after this time was based on the patient clinical course or individual clinician preference. Cases in which complications developed were generally managed by minimally invasive approaches in the first instance. Term quality of life measures when the patients back to work within two weeks after discharge or not and their satisfaction score after surgery (score 1 for being totally not satisfied with surgery and 10 for being satisfied with surgery).
3. Result
- Fifty five (67.07%) patients were on operative management while 27 (32.93%) were on conservatively management. The common organ detected using CT scan on the patient were bowel (23%) injury followed by liver injury (21%) and splenic injury (19%) (Figure 1).
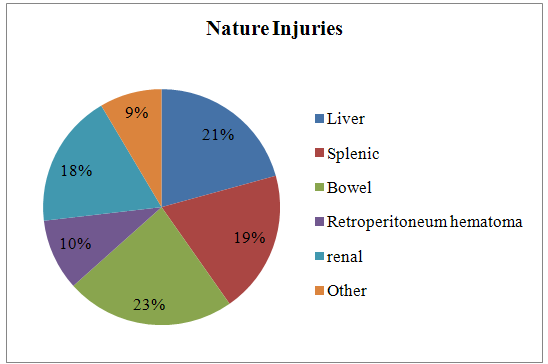 | Figure 1. Distribution of Intra-Abdominal Nature Injuries |
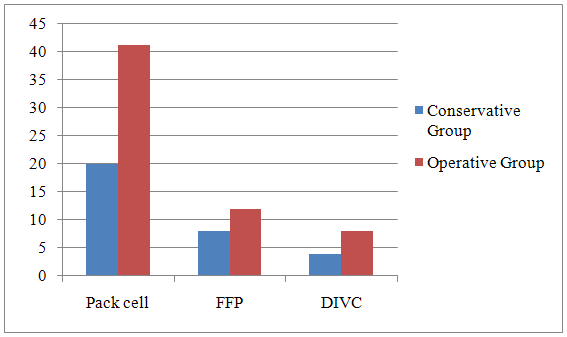 | Figure 2. Usage of Blood Products |
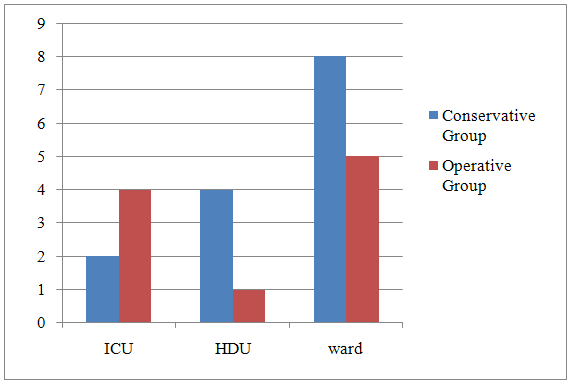 | Figure 3. Length of Stay in Hospital |
4. Discussion
- This study included eighty two patients who had developed solid organ injury due to motor vehicle accident and bought to Hospital USM. Incidence of road traffic as a cause of solid organ injuries in this study was matched with that was found in Indian study [6].Present study detected bowel as the common solid organ injury. While in previous studies founded spleen and liver as the common organ injury [6-8]. There is no evidence to note that complete bed rest for non operative patients confer any benefit [9-11]. There was contradict results with previous study when present study showed patients that were conservatively managed had significant longer hospital stay [6]. While in Pakistan, study revealed that patients in whom conservative management failed had longer length of hospital stay compared to patients who were managed successfully without operation [12].For penetrating abdominal injury, it is recommended to use conservative management with good facilities, resources and experience to monitor patients with penetrating abdominal injury carefully, along with the capability to provide immediate surgical intervention to those who need it. Patients that were managed conservatively or operatively did not vary very much in terms of mortality. Failure in conservative management were more likely due patient with severe injuries, requiring blood transfusion and those with splenic injury [12]. Commonly in the USA, CT scan is performed when conservative management is being considered for patients. From meta-analysis study, the accuracy of CT scan was found 97.70 per cent in determining the need for laparotomy in haemodynamically stable patients with penetrating abdominal injury [13]. No association was found between abdominal CT scan and failure or success of conservative management since there was not much varies in mortality outcome between two management. Further prospective study may be needed for the evaluation of the role of CT scan in selecting patients with intra-abdominal injury for conservative management. It is recommended that the appropriate infrastructure of a emergency and accident unit combined with an experienced surgical group and established protocols for 24 hour monitoring were the key components for success of conservative management [14]. Conservative management of intra-abdominal injury is feasible however a CT scan is mandatory before conservative management can be undertaken. When considering conservative management for intra-abdominal injury, the ability to monitor patients carefully and providing appropriate operative intervention when needed must be ensure first. Factors such as the need of blood transfusion and injury severity should identified when selecting patients for conservative management, as the effects of failure are not inconsequential. In addition, selected patients for conservative management are expected to be observed and to undergo serial physical examinations by experienced clinical staff [15, 16]. It Frequent assessments for changes in examination findings or development of peritoneal signs at regular intervals are mandatory, so that injuries are diagnosed as soon as they are clinically apparent.
5. Conclusions
- Intra-abdominal injury is one of major cause of morbidity and mortality. Choosing between operative or conservative management for intra-abdominal injury is crucial part to improve the treatment outcome. Ultrasonography and CT scan allow physician to use less surgery because they can identify injuries that can be managed conservatively and rule out others injuries that need surgical treatment.