-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2015; 5(1): 7-9
doi:10.5923/j.ajmms.20150501.02
Periodontal Status of Children with Dental Fluorosis in Juja, Kenya
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLLucy W. Waweru1, Harun Kimani2, Opinya G. N.3, Ng'ang'a P. M.3
1Department Paediatric Dentistry, University of Nairobi, Nairobi, Kenya
2Department of Community Health, School of Public Health, Kenyatta University, Nairobi, Kenya
3Department of Paediatric Dentistry and Orthodontics, Faculty of Dental Sciences, University of Nairobi, Nairobi, Kenya
Correspondence to: Harun Kimani, Department of Community Health, School of Public Health, Kenyatta University, Nairobi, Kenya.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
The objective was to determine the periodontal status of children with dental fluorosis. This was done through a descriptive cross sectional study with the aim of determining the periodontal status of children aged with dental fluorosis from a rural area in Kenya. The area was purposively selected as ground water was major source of domestic water. Simple random sampling technique was used to select the school. Statistical tests done included chi-square test, odds ratio to determine the association of periodontal status of children with fluorosis and those without. Results showed that of 225 children who were included in the study of these 125 were males and 100 were females with a mean age of 13.28 ±1.1 standard deviation. Dental fluorosis was present in 114 (50.7%) of the study population as measured by Thylstrup and fejerskov Index (TFI). 51.9% scored TFI score 0, while 41.4% scored TFI score 1-4 and 8.7% scored TFI score > 5. The fluoride level in the surface water was 0.2 ppm and 3.6 ppm in the borehole water. The distribution of Community Periodontal Index (CPI) scores among the children showed that CPI score 0 (healthy) CPI Score 1 (gingivitis) and CPI scores 2 (gingivitis + calculus) were present in 24.4%, 51.6% and 24% respectively. In conclusion children with fluorosis had a higher prevalence of gingivitis and there was a statistical significant difference in the occurrence of gingivitis in all sextant except the lower anterior when the teeth with fluorosis and those without fluorosis were compared. The more severe the level of fluorosis the higher was the risk of gingivitis.
Keywords: Dental Fluorosis, Gingivitis, Children, Kenya
Cite this paper: Lucy W. Waweru, Harun Kimani, Opinya G. N., Ng'ang'a P. M., Periodontal Status of Children with Dental Fluorosis in Juja, Kenya, American Journal of Medicine and Medical Sciences, Vol. 5 No. 1, 2015, pp. 7-9. doi: 10.5923/j.ajmms.20150501.02.
1. Introduction
- Fluoride has been shown to have a role in the clinical and microscopic manifestation of dental flurosis. Epidemiological studies have given contradictory findings concerning the relationship between periodontal disease and dental fluorosis [1, 2]. A study done among populations in the low and high fluoride areas of Morocco showed that the subjects in the high fluoride area had a lower prevalence of periodontal disease as compared to the low fluoride area. The author hypothesized that the antibacterial effect of fluoride on suspected plaque periodontal pathogens might favorably influence the balance of defense in periodontal tissues. In Hungary no difference was reported in the oral hygiene status and gingivitis between children living in a high fluoride city (1.7 ppm – 2.00 ppm) and a low fluoride area (7.0 sppm) Albrecht et al. There is paucity of information concerning the prevalence and severity of periodontal disease in high fluoride areas in Kenya.
2. Materials and Methods
- 225 primary school children aged 12-15 years were included in the study. These ages were important as this was the last time that a sample can be obtained through the primary school system before they leave the schools. At the ages of 12-15 years most of the permanent teeth have erupted and also the post eruptive changes of dental fluorosis have taken place. The age of 15 years is important in assessing the periodontal health in adolescence. A questionnaire was used to elicit if the children were born in the area. The main source of water used by the respondents was elicited indicating if they used borehole or surface water. The study community was selected as it was a migratory worker population hence it was possible to get children in the same community without dental fluorosis. The two group who were currently living in the same community reduced the confounding factor.A sampling frame was developed and a table of random numbers was used to randomly select the school. Pupils in class five, six, seven and eight were selected and all individuals in the cluster who met the inclusion criteria and consented to participate in the study were recruited. Oral examination was done in one of the classrooms using natural light. Dental probes and mirrors were used for examination – the community periodontal index was used to score for periodontal disease.
3. Results
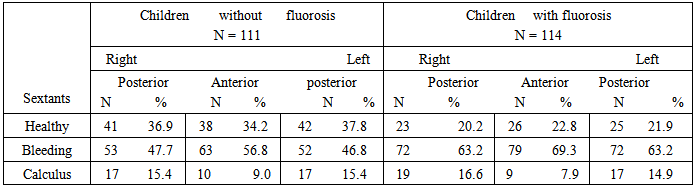
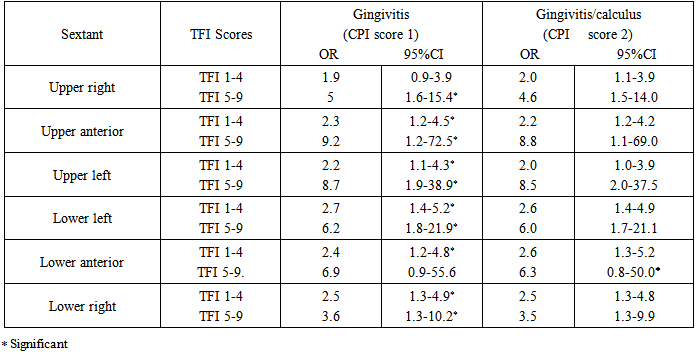
- The percent number of children who had healthy gingival was 24.4% while 51.6% had bleeding gingival, calculus was present in 24% and none of the 15 year olds had any pockets. Bleeding gingival was more prevalent among the children with fluorosis as compared to those without fluorosis. Among the children with fluorosis the number of sextant with bleeding was 63.2% in the upper right 69.3% in the upper anterior and 63.2% in the upper left. While among the children without fluorosis bleeding was present in 47.7%, 56.8% and 46.8% of the sextants in the upper right, upper anterior and upper left respectively, and calculus was most prevalent in the upper posterior sextant 16.6% among the children with fluorosis.The risk of having gingivitis among all the index teeth was higher when the TFI scores was 5-9 than when the score was TFI score 1-4. The odds ratio for tooth type 16, 11, 26, 36, 31 and 46 were 1.9, 2.3, 2.2, 2.7, 2.4 and 2.5 respectively with the TFI score 5-9 they were 5.0, 9.2, 8.7, 6.2, 6.9 and 3.6 respectively. There was a statistical significant relationship between dental fluorosis and periodontal disease in all the index tooth except in the upper right quadrant when CPI score I was related to the TFI score 1-4, in the lower anterior sextant where CPI score 2 was related to TFI score 5-9.
4. Discussion
- Periodontal status was assessed using the CPI index. The indicators used to assess periodontal status, were bleeding, calculus and periodontal pockets. In the study population 51.6% of the children had bleeding and 24.4% had calculus in at least one of the sextant. The mean sextants with gingivitis were 3.5, gingivitis was present in 75.6% of the sample population and the mean sextant with calculus in the study population was 0.74. The teeth which scored TFI scores 5-9 showed a higher risk of gingivitis when compared to TFI score 1-4 with a statistical significant difference in the occurrence of gingival bleeding and calculus in the two groups. The difference could be explained by the fact that the pitting of enamel and loss of tooth structure in TFI score 5-9 could have contributed to more plaque relation as well as in difficulties in maintaining good oral hygiene. Albrecht et al [3] reported no difference in the oral hygiene status and gingivitis among children in high and low fluoride cities in Hungary.
|
|
5. Conclusions
- There was an association between periodontal disease and dental fluorosis. The prevalence of gingivitis was 75.6%.