-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2014; 4(6): 212-215
doi:10.5923/j.ajmms.20140406.03
Levels of Highly Sensitive C-reactive Protein and Gamma-Glutamyltransferase in Sudanese Patients with Metabolic Disorders
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLHassan A. Elahiekh1, Alfatih S. Aljafari2, Abd Elkarim A. Abdrabo1
1Department of clinical chemistry, faculty of medical laboratory science, Alneelain University-Sudan
2Pathology Dept-College of Medicine-Aljouf University, KSA
Correspondence to: Abd Elkarim A. Abdrabo, Department of clinical chemistry, faculty of medical laboratory science, Alneelain University-Sudan.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
Objectives: The objective of this study is to evaluate the levels of gamma-glutamyltransferase and highly sensitive C-reactive protein in patients with metabolic disorders in Sudan. Material and method: A case control hospital based study was carried out at Atbara-River Nile State-Sudan. Total of 294 participants, 194 patients were with at least one of the metabolic disorders (Diabetic, Obese, or Hypertensive) were enrolled in this study together with 100 healthy control subjects during the period from October to November 2013. For all participants, body mass index (BMI), gamma-glutamyltransferase (GGT) and highly sensitive C-reactive protein (hs-CRP) were measured using standard methods. Result:A significant elevation of GGT levels was observed in all patients (diabetic, hypertensive, and obese). Levels of hs-CRP significantly increased in obese and diabetic. While in hypertensive patients insignificant elevation was observed. Conclusion: patients with metabolic disorders, included in this study, have significantly elevated GGT levels and hs-CRP except hypertensive.
Keywords: DM, HTN, Obesity, GGT, hs-CRP, BMI
Cite this paper: Hassan A. Elahiekh, Alfatih S. Aljafari, Abd Elkarim A. Abdrabo, Levels of Highly Sensitive C-reactive Protein and Gamma-Glutamyltransferase in Sudanese Patients with Metabolic Disorders, American Journal of Medicine and Medical Sciences, Vol. 4 No. 6, 2014, pp. 212-215. doi: 10.5923/j.ajmms.20140406.03.
1. Introduction
- Metabolic syndrome (MetS), also known as dysmetabolic syndrome, refers to a cluster of metabolic conditions that can lead to heart disease [1].There are five conditions which considered as metabolic risk factors. Large waistline "abdominal obesity", high triglyceride level, high blood pressure, high fasting blood sugar, and low HDL cholesterol level [2].In Africa, the burden of cardiovascular disease is increasing rapidly and it is now a public health concern. The most important cardiovascular diseases in the African region are those related to hypertension, atherosclerosis, cardiomyopathies and rheumatic heart disease [3]. A previous study done in Sudan reported a high prevalence of diabetes in the adult population, with a wide difference among the different areas [4]. Percentages of diabetic complications were as follows: neuropathy 28.1%, retinopathy 18.5%, cataract 14.7%, hypertension 12.9%, nephropathy 11.6%, peripheral vascular disease 6.2%, coronary heart disease 4.2% and pulmonary tuberculosis 2.7% [5].C-reactive protein (CRP) is a plasma protein synthesized in liver. It is induced by cytokines produced by accumulated adipocytes. It is a sensitive inflammatory marker and it is likely associated with cardiovascular disease (CVD) [6]. Inflammation plays an important role in the development of disturbances in both glucose metabolism and CVD [7]. It had been hypothesized that elevated CRP levels contributes to increased cardiovascular risk (8). Festa et al. reported that CRP was positively correlated with considerable components of MetS, such like body mass index (BMI), waist circumference, blood pressure (BP), triglycerides, cholesterol, LDL cholesterol, plasma glucose, and fasting insulin, and then increases in subjects with metabolic syndrome [9]. Gamma glumly transferee (GGT) is a protein found in many tissues, has a particular affinity as marker of liver dysfunction, making it invaluable as diagnostic marker for hepatobiliary diseases [10;11], Recent reports suggested that, elevated GGT is associated with atherogenesis and oxidative stress, making it a target marker for coronary disease and risk of stroke [12]. It has been shown that GGT expression becomes more apparent by oxidants, suggesting that increased GGT activity may be a marker for oxidative stress [13]. Previous study reported that patients with MetS have a higher serum GGT activity than those without this syndrome [14]. The aim of this study is to evaluate serum GGT activity and hs-CRP concentration in Sudanese patients with metabolic disorders.
2. Material and Method
- This is a case-control hospital based study of a qualitative and quantitative approach. The study was conducted at Atbara Teaching hospital and Atbara medical complex, in the period from October to November 2013. A total number of 294 adults (male and female) participants were enrolled in this study. One hundred sixteen of them were with one metabolic disorder, diabetic (no=63), high blood pressure (no=62), or obesity (no=69) BMI >30, together with hundred apparently healthy adults as control. Volunteers were fully informed of the nature and purpose of study. Total persons had baseline information of smoking, alcohol abuse and CVD exposure. Pregnant ladies and patient demonstrating urinary tract infection or known cases of chronic kidney disease were excluded from the study.Biochemical measure: venous blood was collected into plain tubes, GGT and hs-CRP levels were measured using (A25 Biosystem®) chemistry analyzer. Statistical analysis: data were expressed as mean and standard deviation (M±SD), the means were compared using independent sample T. test, Persons correlation analysis was used for correlation of parameters measured, P-value < 0.05 was considered as statistically significant.
3. Results
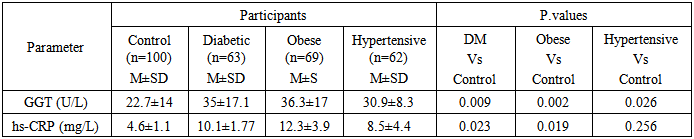
- One hundred and sixteen Sudanese subjects were enrolled in the study, diabetic subjects, hypertensive, and obese (BMI was above 30) matched for age and gender with 100 normal controls. The mean age of participants was (45.4±13.4) years, 145 female and 151 male.The mean of GGT activity of diabetic subjects were significant higher (35±17.1 U/L), compared to control subjects (22.7±14 U/L), P < 0.05. The mean values of hs-CRP in diabetic were rending to be significantly higher (10.1±1.77 mg/L) than control (4.6±1.1 mg/L), P < 0.05.Gamma GT levels among obese subject were significantly higher (36.3±17) compared to control subject (22.7±14 U/L), P < 0.05. There is a tendency of hs-CRP to increase among obese (12.3±3.9 mg/L) compared to control (4.6±1.1 mg/L) P < 0.05. Gamma GT levels of hypertensive subjects were significant higher (30.9±8.3 U/L) compared to control subjects (22.7±14 U/L), P < 0.05. The mean values of hs-CRP in hypertensive were higher (8.5±4.4 mg/L) than the values in control (4.6±1.1 U/L) but the difference did not achieve significant values P > 0.05.
4. Discussion
- The findings of this study revealed that there were increased levels of GGT, oxidative stress marker, and hs-CRP, systemic inflammatory marker, among study population. Studies which have examined the link between GGT and CRP as markers of MetS have generally found a positive association [14-16], one study found that elevated levels of GGT and high sensitivity CRP had a synergistic effect and were associated with the MetS and insulin resistance [14], these markers could be strong predictors for metabolic disorder as had been suggested in previous literature [17, 18]. There are only few of studies that have assessed the relation between GGT and CRP and the risk of developing metabolic disorder. Although the findings in this study were statistically significant, it is not fairly enough to say that these biomarkers (GGT and CRP) are produced during developing an abnormal metabolic profile and then CVD, because they may increase in patients with liver dysfunction and inflammation which are consequence results of unhealthy lifestyle.Although the exact mechanism responsible for this association is unknown, the finding of the current study confirms the data which indicate that there is an association between serum GGT levels (within the normal range) and cardiovascular diseases [19].Elevated serum Alanine amino transferase (ALT) and GGT are markers of non-alcoholic fatty liver disease (NAFLD) [20], which is thought to cause hepatic insulin resistance and CVD [21], but only GGT activity has been reported to be related to oxidative stress [22].Oxidative processes are components of chronic inflammation acting on different pathways and stimulating the inflammatory response [23], and it has been shown that an association exists between inflammatory process and CRP level, so an association might exists between serum GGT and CRP levels. The current results found elevated levels of these markers in diabetic and obese individuals. This finding is important in that increased GGT activity is associated with an inflammation marker.
- The increased GGT activity in diabetic patients of this study confirm the findings of Nakanishi et al, who reported that GGT activity was related to the development of impaired fasting glucose or type 2 DM [24].GGT was introduced in routine investigations in Sudan to asses liver function and CRP as inflammatory marker, but now the outcome of this study and other studies confirm that these markers are becoming an important addition to the multimarker approach to cardiovascular risk evaluation.
5. Conclusions
- The present study showed that hs-CRP and GGT levels are strongly associated with obesity and diabetes; while in hypertensive patients there is a significant higher levels of GGT in with insignificant elevation of hs-CRP.