-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2014; 4(5): 186-191
doi:10.5923/j.ajmms.20140405.09
Alanine Aminotransferase and Gamma-glutamyltransferase Activity as Predictor Markers for Hepatocellular Damage in Vitamin D Deficient Type 2 Diabetes Mellitus Patients – Cross-sectional Study
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLNihal Magzoub Yousif1, Amar Mohamed Ismail2
1Department of Clinical Chemistry, Faculty of Medical Laboratory Science, AL-Neelain University, Sudan
2Department of Biochemistry & Molecular Biology, Faculty of Science and Technology, AL-Neelain University, Sudan
Correspondence to: Amar Mohamed Ismail, Department of Biochemistry & Molecular Biology, Faculty of Science and Technology, AL-Neelain University, Sudan.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
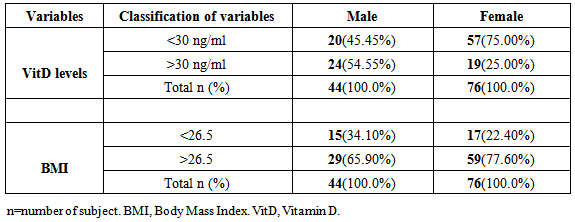
Background: GGT known as strong predictor of risk factor of DM, and there is association between ALT and insulin resistance, however vitD has important role in modifying risk factors of DM, therefore present study aims to evaluate the ALT and GGT activity as markers for hepatocellular damage in vitD deficient type2 diabetes mellitus patients.Materials and methods: Descriptive cross-sectional study, 120 type2 DM patients were enrolled in this study, then classified into two groups based on vitD results, <30 ng/ml considered as cases and >30ng/ml as control. Fasting blood samples were collected and VitD, ALT, GGT and glucose level were estimated using competitive ELISA kit, and kinetic spectrophotometry method.Results: DM is more common in females76 (63%) than in males44 (37%). 57 (75%) of DM females and20 (45.45%) of DM males were suffering from vitD deficient, 59 (77.60%) female have over weight (BMI >26.5) compared with 65 (65.90%) male. VitD deficient is more common in over weight male 15 (51.72%), in contrast vitD deficient observed in both normal and overweight 11 (64.71%) and 46 (77.96%) females. There was significant increase in GGT (P-value 0.038), and no significant difference in ALT activity (P-value 0.067) in vitD deficient patients, there was week negative correlation between GGT and ALT versus vitD (-0.183) and (-0.127) respectively.Conclusions: Study concludes DM females were more vulnerable to vitD deficient than males. DM patients with vitD deficient tend to have higher ALT and GGT. Therefore, could beuseful predictor markers for hepatocellular damage and cholestasis in vitD deficient DM patients.
Keywords: ALT, GGT, Vitamin D deficient, Type2 DM
Cite this paper: Nihal Magzoub Yousif, Amar Mohamed Ismail, Alanine Aminotransferase and Gamma-glutamyltransferase Activity as Predictor Markers for Hepatocellular Damage in Vitamin D Deficient Type 2 Diabetes Mellitus Patients – Cross-sectional Study, American Journal of Medicine and Medical Sciences, Vol. 4 No. 5, 2014, pp. 186-191. doi: 10.5923/j.ajmms.20140405.09.
Article Outline
1. Introduction
- Diabetes mellitus is a group of metabolic diseases characterized by high blood glucose results from defects in insulin secretion, its action, and/or both, there are two major types of diabetes type 1 and type 2 [1] the prevalence of diabetes for all age groups worldwide was estimated to be 2.8% in 2000 and 4.4%in 2030, the total number of people with diabetes is projected to rise from 171 million in 2000 to 366 million in 2030 the most important demographic change to diabetes prevalence across the world appears to be the increased in the proportion of people >65 years of age [2], diabetes is an increasing cause of death in developing countries [3].The liver is an important organ for glucose metabolism; this includes glucose uptake, storage, and synthesis [4]. Alanine aminotransferase (ALT) and γ-glutamyltransferase (GGT) were strongly associated with obesity, insulin resistance, and the metabolic syndrome, elevated GGT and ALT enhanced the prediction of diabetes risk [5]. Non-alcoholic fatty liver disease (NAFLD) increases the risk for the type 2 diabetes mellitus, serum ALT has been closely correlated with liver fat accumulation, therefore, this enzyme is commonly used as a biomarker of NAFLD, in addition, studies have associated serum ALT levels with insulin resistance, the metabolic syndrome and the development of type 2DM. Insulin normally inhibits hepatic glucose production, therefore, elevated fasting insulin can be considered a surrogate marker of hepatic insulin resistance [4].Elevated activities of serum GGT are shown to be a strong predictor of type 2 diabetes mellitus independent of obesity index, while hepatic steatosis associated with visceral adiposity may be a common mediator for elevated GGT and insulin resistance [6]. GGT is a plasma membrane enzyme involved in the so-called gamma-glutamyl cycle by which extracellular glutathione is transported into cells for the synthesis of intracellular glutathione, oxidative stress results in an increase in GGT so that the redox regulation is maintained [7]. Interestingly, it was shown that a decreased risk of type 2 diabetes associated with coffee consumption was more pronounced in individuals with elevated activities of serum GGT [6], the risk of having a high level of ALT or GGT tended to be higher for lower vitD levels [8].Vitamin D is a fat-soluble vitamin that plays an important role in bone metabolism and seems to have some anti-inflammatory and immune-modulating properties [9]. VitD receptors are present in both pancreatic beta-cells and immune cells, beside its classical role as the major regulator for calcium absorption, vitD mediates the activity of beta-cell calcium-dependent endopeptidases promotes conversion of proinsulin to insulin and increases insulin Output [10], accordingly vitD deficiency may be associated with type 2 diabetes, vitD sufficiency may provide protection against type 2 diabetes vitD deficiency is thought to be a risk factor for development of type 2 diabetes, although the underlying biological mechanisms are poorly understood, the association of low serum 25-hydroxyvitamin D3 [25(OH) D3] concentrations with type 2 diabetes may be mediated through effects on glucose homeostasis and, in particular, a direct effect of vitD on the beta-cell function, and thus insulin secretion. Several studies have suggested that low vitD status also contributes to insulin resistance thus low vitD status is associated with markers of impaired glucose metabolism [11].
2. Materials and Method
- Cross-sectional study was conducted at primary Health Care Center (Almotakamil) in Khartoum state, during the period from May to July, 120 type2 DM patients 44 were males and 76 were females aged between 25-80years were enrolled in this study, classified based on vitD results into two groups, <30ng/ml as case group and>30 ng/ml as control group. Overnight fasting blood specimens were collected, and then centrifuged at 3000rpm for 10min and serum stored at −20°C till utilized.
2.1. Ethical Consideration
- The study has been approved by the local ethics committee of Al-Neelain University. Written informed consents were obtained and all participants were informed by the aims of study. Sample and clinical information were used anonymously.
2.2. Measurement of BMI
- Weight and height were measured and BMI was calculated by dividing weight in (Kg) by squire of height in (m).
2.3. Estimation of Vitamin D
- Briefly according to manufactured, competitive inhibition enzyme immunoassay was used to determine vitD (Elisa kit lot E 140116AE) (EuroIMMUN AG) Germen, 200µl of sample diluted with biotin microplate well which coated with monoclonal anti-vitD antibodies, after incubation antigen antibodies reaction occurred, then unbounded 25-OH vitD was removed by washing,100µlof streptavidin-peroxidase added for detection of bond biotin labelled 25-OH vitD, 100µltetramethylbenzidine substrate was added, color intensity is inversely proportional 25-OH vitD concentration in the sample, sample calculated using plotted standards curve sunrise-TECAN) [12, 13].
2.4. Estimation of Glucose
- Glucose oxidase catalyzed oxidation of beta D-glucose present in the plasma to glicono-1, 5-lactose then hydrogen peroxide was formed, which react with 4-aminoantipyrine and phenol formed quinoneimine color, then absorbed at 546 nm using spectrophotometer BTS-310 Biosystem, the concentration obtained by calculation of O. D of test against O. D of standard, 10 µl of serum was added to 1ml of working reagent then mixed and incubated for 10 min [14].
2.5. Estimation of ALT
- Alanine aminotransfease catalyzed the reversible transaminase of L-alanine and α-oxoglutarate to pyruvate and L-glutamate, the pyruvate was then reduced to lactate in presence of lactate dehydrogenase (LDH) with the concurrent oxidation of reduced B-nicotinamide adenine dinucleotide (NADH) to B-nicotinamide adenine dinucleotide (NAD), this change in absorbance is directly proportional to the activity of ALT in the sample, 100µl of serum was added to 1000µl of working reagent, then ΔA/time measured interval, using spectrophotometric method BTS-310 Biosystem [15].
2.6. Estimation of GGT
- Gamma-glutamyltransferase transfer the gamma-glutamyl group of gamma-glutamyl-3-carboxy-4-nitroanilide to glycyl-glycine with the production of p-nitroaniline, the amount of 5-amino-2-nitrobenzoate result in the elevated absorbance which is directly proportional to the activity of GGT in the sample, 100µl of serum was added to1000µlGGT working reagent then ΔA was measured in interval time using spectrophotometer BTS-310 Biosystem [16].
2.7. Statistical Analysis
- Data from all patients were presented as percentage and (mean±SD), differences between means of patients and control groups were considered statistically significant with p-value threshold <0.05 using independent T-test. Significant correlation (r) was calculated using linear correlation test.
3. Results
- Frequency of subjects by gender
|
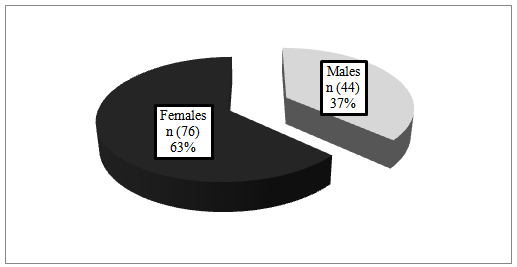 | Figure 1. Shows percentage of males and females among type2 DM patients (n=120) |

 | Figure 5. Shows mean ALT activity in vitD deficient type2 DM patients (16.00±2.30 U/l) compared control group (14.19±0.86 U/l) with in significant difference (P-value <0.067) |
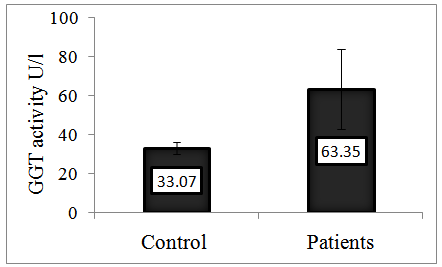 | Figure 6. Shows mean GGT activity in vitD deficient DM patient (63.35±20.48 U/l) compared with control group (33.07±2.94) with significant increase in GGT levels (P-value = 0.038) |
|

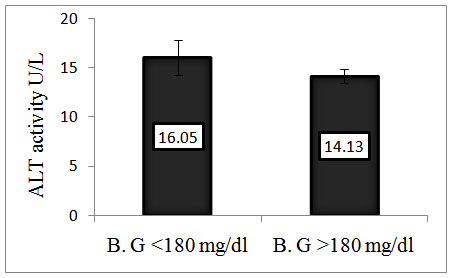 | Figure 7. Presenting mean ALT activity in patients with blood glucose < 180 mg/dl (16.05±1.8 mg/dl) in comparison with those have blood glucose > 180 mg/dl (14.13±0.72) with in significant difference (P-value >0.05) |
 | Figure 8. Presenting mean GGT activity in patients with blood glucose <180 mg/dl (53.92±16.35 mg/dl) in comparison with those have blood glucose>180 mg/dl (32.24±2.88) with significant decrease (P-value <0.05) |
4. Discussion
- Diabetes has become a major public health problem in the general population and increasing worldwide due to change in life style [17], since resent research found relationship between vitD and DM in addition there is association between type2 DM with ALT and GGT, accordingly present study aim to evaluate ALT and GGT in vitD deficient type2 DM patients. The results of frequency showed the percentage of type2 DM is higher among females (63%) than males (37%), which agree with study done by Marina in India who reported the prevalence of diagnosed type2 DM was higher among female than male, also separate reports have stated vitD deficiency is common among female [18, 19]. In addition our study observed that the percentage of vitD deficiency is common among female (75%) than male (45.45%), these results suggested that females are more vulnerable to vitD deficiency than males. Since hypovitD is risk factor for type2 DM in both female and male and in fact that vitD have role in glucose homeostasis, insulin resistance and cells damage [20], our study explain that DM females are more susceptible to the complications of vitD deficient than type2 DM male.Previous reports have shown that, type2 DM female patients were more overweight than male [21], Based on mentioned stated our results revealed that percentage of overweight was slightly higher in DM female (77.60%) compared with DM male (65.90%). Also our study observed that, overweight male tend to have vitD deficient (51.72%) than normal weight male (33.30%), in contrast both normal and overweight female have shown high percentages of vitD deficient (64.71%) and (77.71%) respectively, which explain the association between BMI and vitD level in males, withno evidence of relation between BMI and vitD level observed in females. Subsequently our finding agreed with Ehsaneh who stated that there is negative relationship between vitD and BMI adjusted for gender [22]. Based on previous studies justification that, supplementation of vitD reduces concentration of free fatty acids in patients with type2 DM improve insulin sensitivity and reduce BMI. To our knowledge the current study is first to evaluate GGT and AST activity in type2 DM patients with vitD deficient, as GGT marker for cholestasis and ALT for hepatic jaundice, our results provide evidence that GGT activity significantly increased in type2 DM with deficient vitD patients when compared with normal vitDtype2 DM patients with (p-value 0.038), and in significant difference in ALT with (p-value 0.067) respectively, which reinforced by person’s regression results of week negative correlation between vitD versus GGT (r -183) and ALT (r -127). Based on previous report that the risk of having high level of ALT or GGT tended to be higher for lower vitD level [8]. This indicated that type2 DM patients with vitD deficient are more susceptible for hepatocellular damage and cholestasis. Since interaction between vitD and its receptors response elements in the promoter region of cytokine genes to interfere with nuclear transcription factors implicated in cytokines generation and its action and can downregulate activation of NFkB, thus prevent the damage of tissues [20]. The present study observed that, there was decreased in mean ALT and GGT activity in type2 DM patients who have blood glucose>180mg/dl compared with those have blood glucose <180 mg/dl, which may be due to hyperosmolar caused by high blood glucose, leading to haemodilution, which may result in decease ALT and GGT activity.
5. Conclusions
- Study concludes type2 DM female was more susceptible to vitD deficient than male.Type2 DM patients with vitD deficient tend to have higher ALT and GGT. Therefore ALT and GGT could be measured as predictor markers for hepatocellular damage and cholestasis in vitD deficit type2 DM patients. Further studies are required to understand underlying mechanisms.
Abbreviations
- DM, Diabetes Mellitus; VitD, Vitamin D; ALT, Alanine Aminotransferase; GGT, Gamma Glutamyltransferase.
References
| [1] | Melissa Conrad Stoppler., (2014), diabetes mellitus. Medicin Net.14; 2. |
| [2] | Sarah wild, Gojka Roglic, Anders Green, Richard Sicree and Hilary King., (2004), Global prevalence of diabetes Estimates for the years 2000 and projection for 2030.Diabetes care .27; 1047-1053. |
| [3] | Valeria Maria de Azeredo Passos, Sandhi Maria Barrelo, Leonardo Maurico Diniz, Maria Fernando Lima-Costa. Type-2 Diabetes: Prevalence and Association Factors in Brazilian Community the Bambi Health and Aging Study. Sao Paulo Medical Journal. 2005; 123(2): 66-71. |
| [4] | Miguel Angel Gomez Samano, Danile Cuevas-Ramos, Roopa Mehta, Hasan Brau- Figueroa, Clara Elena Meza- Ararna and Alofonso Gulias-Herrero., (2012), Association of Alanine Aminotransferase level (A LT) with The Hepatic insulin Resistance index (HIRI): across-sectional study. BMC Endocrine disorder. 9; 1472-6823. |
| [5] | Sasiwarang Goya Wannamethee, Andrew Gerald shaper, Lucy Lennon and peter H-Whincup., (2005), Hepatic enzymes, The Metabolic syndrome, and The Risk of Type 2 diabetes in older men .diabetes Care.28; 2913-2918. |
| [6] | Zhenjie Wang, Christopher MC Monagle, Shinichiro Yoshimitsu, Sanjeev Budhathoki, Makiko Morita, Kengo Toyomura, Keizoohnaka, Ryoichi Takayanagi and Suminori Kono., (2012), No effect modification of serum bilirubin or coffee consumption on The association of gamma-glutamyltransferase with glycated hemoglobin in across-sectional study of Japanese men and women.BMC, Endocrine disorder.7;1472-6823. |
| [7] | Richard A. Hawkins, Darryl R. Peterson, and Juan R., (2002), the Complementary Membranes Forming the Blood-Brain Barrier. IUBMB Life.54; 1-7. |
| [8] | Skaaby T, Husemoenll, Borggglykke A, Jorgensen T, Thuesen BH, Passenger C, Schmidt LE and Linneberg A., (2013), vitamin d status, liver enzymes and incident liver disease and Mortality: a general population study. Endocrine journal.1-6. |
| [9] | Teresa Kulie, Amy Groff, Jackie Redmer, Jennie, Hounsheil and Sarina Schrager., (2009), Vitamin D: An-Evidence –Based Review. The American Board OF Family Medicine. 22; 698-706. |
| [10] | Krishna G Seshadri, BubbLU Tamilselvan, Amarabalan Rajeudran, (2011), Role of vitamin D in Diabetes. Journal Endocrinal Metab.10; 47-56. |
| [11] | Christine Dalgard, Mania Skaalum Petersen, Palweihe And Philippe Grand jean., (2011), vitamin d status in relation to Glucose Metabolism and Type2diabetes in septuagenarians. Diabetes care.34; 1284-128. |
| [12] | Holick MF, Chen TC, (2008), Vitamin d deficiency: a worldwide problem with health consequences. Am jClinNutr.87; 1080-1086. |
| [13] | Hollis Editorial, (2004), The Determination of circulating 25-Hydroxyvitamin D: No Easy Task BW. J ClinEndocrinalMetab.89 (7); 3149-3151. |
| [14] | Trinder P, (1969), Determination of glucose in blood using glucose oxidase with an alternative oxygen acceptor, Ann Clinical Biochemistry.6; 24-27. |
| [15] | Gella F J, Olivella T, Crus Pastor M, Arenas J, Moreno R, Durban R and Gomez J A. simple procedure for routine estimation of aspartate aminotransferase and alanine aminotransferase with pyridoxal phosphate. Clin Chim Acta 1987; 153: 241-247. |
| [16] | Thomas L, (1998), Alanine aminotransferase (ALT), Aspartate aminotransferase (AST). in: Thomas L editor. Clinical Laboratory diagnostic1st.Frankfurt: TH-Books verlagsgesellschaft.55-65. |
| [17] | Syed Amin Tabish., (2007), is Diabetes Becoming the Biggest Epidemic of the Twenty-first century. International journal of Health science.1; 1-9. |
| [18] | Abdulkaream O, Yousif M, Abdula A, Dejanb H, Fays F, Ali S, Abdulrahaman A, Bharati V and Ajay K., (2013), Prevalence of vitamin D deficiency in Saudi Adults. Sudai Med. 34; 814-818. |
| [19] | Marina Scavini, Christine A, Vallabho, Andrew S, Francesca T, David S, Arlene B, Carleton P, J eanette B, Eunice J, Kathy N, Donica N, Mildred W, Thomas K, Jean W and Philip G., (2014), Prevalence of diabetes is higher among female than male Zuni Indian. American diabetes association Diabetes care, 26; 55-60. |
| [20] | Chih-CheinSung., Min-Tser Liao., Kuo-Cheng Lu., Chia-Chao Wu., (2012), Role of Vitamin D in Insulin Resistance. Journal of Biomedicine and Biotechnology.2012; 1-12. |
| [21] | Alnasri H A and Ahmed A M., (2008), Patterens of lipid changes among type2 diabetes patients in Sudan. Eastern Mediterranean health journal.14; 314-32. |
| [22] | Ehsaneh Taheir, Ahmed saedisomeolia, Mohmoud D Jalali, Mostafa Qorbani and Manouchehr Madani Civi., (2012), The relationship between serum 25-hydroxy vitamin D concentration and obesity in type2diabetic patients and healthy subject. Journal of Diabetes and metabolic disorder. 11; 1-6. |