-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2014; 4(5): 175-179
doi:10.5923/j.ajmms.20140405.07
Palmar Creases; A Comparative Study between Epilepsy Patients and Healthy Subjects among Hausas of Northern Nigeria
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAminu A. Taura1, Magaji G. Taura2, Lawan H. Adamu2
1Department of Psychiatry, Aminu Kano Teaching Hospitals/Bayero University Kano, Nigeria
2Department of Anatomy, Faculty of Medicine, Bayero University Kano, Nigeria
Correspondence to: Lawan H. Adamu, Department of Anatomy, Faculty of Medicine, Bayero University Kano, Nigeria.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
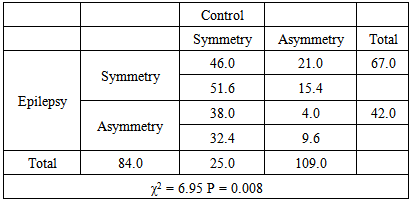
We undertook a comparative study to determine prevalence of normal and abnormal palmar creases, prevalence of asymmetry of palmar creases and association of type of palmar creases between epilepsy patients and a healthy group among the Hausa ethnic group. One hundred and nine (109) epilepsy patients, comprising of 65 males and 44 females of wide age spectrum were recruited. Equal number of undergraduate students participated as controls. Fisher’s exact and Pearson’s chi square test was used to determine the level of association. SPSS version 17 was used for analyses and the level of significance set at P < 0.05. The result shows that there was a higher frequency of abnormal creases in the epilepsy group compared to the control (98.8% against 87%). For abnormal creases, only Suwon creases showed a higher frequency in the control group (3.7% against 2.8%). Also, on the left hand, only normal creases show a higher frequency in the control group (95.4% against 88.0%). Moreover, there was a significantly higher frequency of crease asymmetry among the epilepsy group (38.5 % against 22.9%, χ2 = 6.95, P = 0.008. In conclusion, no significant association was found between type of palmar creases and epilepsy but there is a significantt association in the level of symmetry between the two groups. The significantly higher level of asymmetry in the epilepsy group would suggest that developemental factors that are ralated to epileptogenesis might manaifest as disturbances of palmar crease symmetry.
Keywords: Epilepsy, Hausa, Palmar creases, Symmetry
Cite this paper: Aminu A. Taura, Magaji G. Taura, Lawan H. Adamu, Palmar Creases; A Comparative Study between Epilepsy Patients and Healthy Subjects among Hausas of Northern Nigeria, American Journal of Medicine and Medical Sciences, Vol. 4 No. 5, 2014, pp. 175-179. doi: 10.5923/j.ajmms.20140405.07.
Article Outline
1. Introduction
- Epilepsy has been described as one of the chronic neurological disorders with recurrent unprovoked seizures as one of its typical features [1, 2]. About 90% of world epilepsy populations are living in developing countries [3] Nigeria inclusive. Over several decades dermatoglyphic patterns of the epidermal ridges have been employed as a diagnostic tool for several diseases with strong hereditary background as seen in neurological disorders such as mental retardation [4, 5] and trisomy [6], Down’s syndrome [7], Turner’s syndrome [8], fetal alcoholic syndrome [9] among others. The development of dermatoglyphic features such as the palmar creases relatively begins by the end of the second trimester and remained constant throughout life [10, 11], hence, these features may be a useful indicator of early developmental disturbances in psychosis [12, 13]. The recognition of this fact is possibly behind the high level of interest in dermatoglyphics among psychiatric researchers.Few studies of palmar creases in relation to epilepsy and seizures are quite out-dated and were mostly conducted in non-English speaking countries. Therefore there is aa need to establish a solid niche for dermatoglyphics in an epilepsy research and a specific clinical niche for palmar creases in epilepsy. In order to establish a clinically relevant niche for palmar creases, there is also an obvious need to ascertain their relevance through comparison between the healthy and clinically sick epilepsy patients.We therefore undertook the first stage in the process of bringing back dermatoglyphics into epilepsy research and also making it clinically relevant among Hausas by conducting a comparative study that seeks to determine; the relative prevalence of normal and abnormal palmar creases, the prevalence of asymmetry of palmar creases and association of type of palmar creases between epilepsy patients and healthy group among Hausa ethnic group.
2. Subjects and Methods
2.1. Setting
- The study was based in the North-western Nigeria city of Kano with more than 95% of the population as Hausas. The study population largely comes from the Kumbotso Epilepsy clinic and Bayero University Kano (for control subjects). The clinic was established in 1998 and attends to epilepsy patients on weekly basis, covering wide age spectrum. Diagnosis is mostly clinical with a proportion of patients undergoing EEG and MRI diagnostic investigation.
2.2. Subjects
- One hundred and nine (109) subjects with epilepsy, comprising of 65 males and 44 females were recruited from the attendees of Kumbotso Epilepsy clinic. An equal number of undergraduate students of Bayero University participated in the study as control. The appearance of the palmar creases remain permanent throughout life after their formation in the intrauterine (end of the second trimester) life [10, 11], hence the subjects recruited irrespective of the age category, Subjects with injury to the hand, deformed hands and those who were not of Hausa extraction were excluded from the study. Willing participants who wish to decline their informed consent were also excluded. After the approved informed consent was obtained from the researcher ethical committee of the clinic, basic demographic data were collected from the epilepsy patients and healthy subjects. Three major palmar creases namely; radial longitudinal creases, proximal transverse creases and distal transverse creases were considered in the study. The detailed appearance of the creases was recorded by physical examination as proposed by Dar et al., [14]. The simple classification adopted was based on the relationship between proximal and distal palmar creases which were classified into normal and abnormal creases. The abnormal creases were further classified into three; simian, Sydney and Suwan creases [15, 16]. The level of the symmetry of the crease on both hands was also assessed.
2.3. Data Analyses
- The data was presented using simple percentage to indicate prevalence. The level of association in palmar creases between epilepsy patients and healthy group was determined using Fisher’s exact and Pearson’s chi square tests (where applicable). All analyses were carried out using SPSS version 20 statistical software and differences between the groups were considered statistically significant at P < 0.05.
3. Results
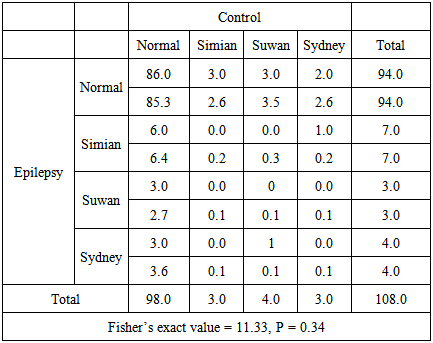
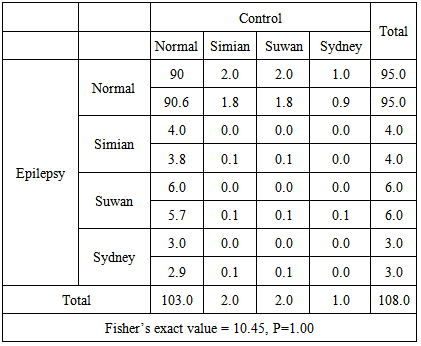
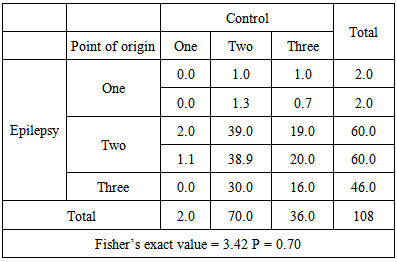
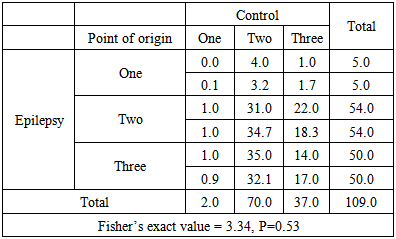
- Comparison of palmar creases of right hand between the epilepsy and control group shows higher prevalence of normal creases in the control group. For abnormal creases only Suwan creases show the higher prevalence in the control group (Fig 1). Similarly on left hand normal creases show higher prevalence in control group but all abnormal creases show higher prevalence in the epileptic group (Fig 2). The data was further presented based on the point of origin of the palmar creases. In figures 3 and 4 the three and one point of origin is higher in both hands among group with epilepsy. In terms of level of symmetry the epilepsy group presented with higher level of asymmetry and low level symmetry (Fig. 5).
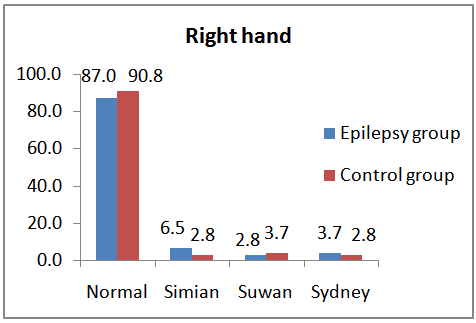 | Figure 1. Comparison of prevalence (%) of types of palmar creases between epilepsy and control groups in the right hand (P > 0.05) |
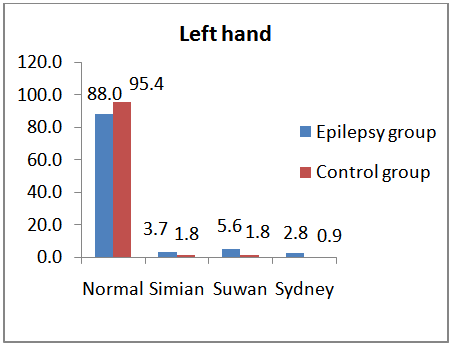 | Figure 2. Comparison of prevalence (%) of types of palmar creases between epilepsy and control groups in the left hand (P > 0.05) |
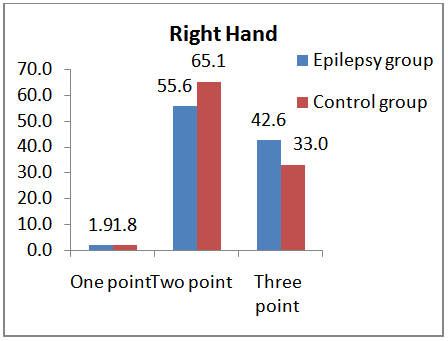 | Figure 3. Comparison of prevalence (%) of types of point of origin of the creases between epilepsy and control groups in the right hand (P > 0.05) |
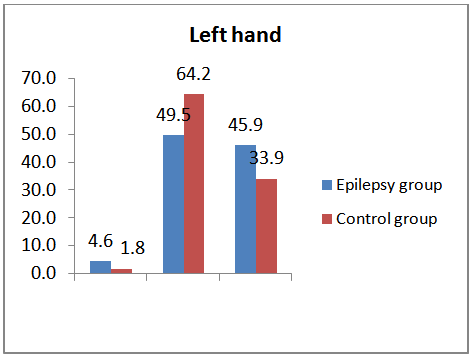 | Figure 4. Comparison of prevalence (%) of types of point of origin of the creases between epilepsy and control groups in the right hand (P > 0.05) |
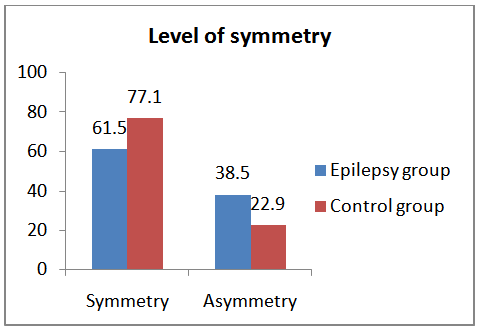 | Figure 5. Comparison of prevalence (%) of creases symmetry between epilepsy and control group (P < 0.05) |
|
|
|
|
|
4. Discussion
- Palmar creases are often useful in discovering anthropologic features and diagnosing number of disease conditions using qualitative [14, 15, 17] and quantitative [18] approaches. Different researchers use different types of classification and methods; therefore comparison of different studies is limited. In the present study we adopted the qualitative approach, simple classification and direct visual inspection to establish the prevalence and association of palmar creases with epilepsy. However, the method adopted may introduce a bias in that some factors may influence how palmar creases are classified [14]. Bias was controlled by ensuring at least two authors agreed on how a given crease is classified. The result shows higher prevalence (98.8% against 87%) of normal creases in the right hand of control group. For abnormal creases only Suwan creases (3.7% against 2.8%) show the higher prevalence in the control group. Similarly in the left hand normal creases show higher prevalence (95.4% against 88.0%) in the control group but all abnormal creases show higher prevalence in the epilepsy group. The data was further presented based on the point of origin of the palmar creases. For three and one point of origin, the epilepsy group had higher prevalence in both hands. In term of level of symmetry the epilepsy patients presented with higher level of asymmetry (38.5% against 22.9%) and low level of symmetry (61.5 % against 77.1). The presence of some abnormal creases in the apparently normal subjects in this study agrees with report of incidence of abnormal creases (especially the simian creases) in population like central Indians [16, 19], Koreans [16], Europeans [20], Nigerians [21, 22] among others. Therefore, we reemphasize the idea that presence of abnormal creases in an individual may not necessarily indicate presence of a disease or syndrome, as it has been noted in apparently healthy people in other studies [20, 23] in different population. Also according to Rodrigues [24], simian creases can be seen in individuals with no more than an average medical condition. However, diagnostic value of abnormal creases was reported in conditions like mental retardation [4, 5] and syndromes like trisomy 21(Down’s syndrome) [6, 7], Turner’s syndrome [8], fetal alcoholic syndrome [9]. Apart from diagnostic application, palmar creases show potential in revealing inter-ethnic variability in anthropometry. Hence, in the current study the participant were drawn from the Hausa ethnic group in order to avoid the influence of the ethnicity on the appearance of the creases. For instance, the frequencies of normal, simian, and Sydney creases are different between Caucasians and Negroes [14], central Indian and Ijaw of Nigeria [19]. Therefore, the existence of abnormal creases alone may not be a good indicator of particular disorders like epilepsy. Probably, there may be a need to determine other abnormal physical characteristics of a subject that may associate with abnormal creases as a screening tool for epilepsy patients. Furthermore, in the current research the level of association of palmar creases was assessed between the epilepsy and control. Significant association (P = 0.008) in the level of symmetry was observed with higher frequency of symmetry association (46 out of 109) then the asymmetry association (4 out of 109). This agrees with evidence of disturbances of symmetry of numerous variables among epilepsy patients [25, 26]. For different types of palmar creases there is no statistically significant association between the epilepsy and control group on both left and right hands. Based on point of origin of palmar creases there is also no statistically significant association between the two groups in this study. When comparing the present finding with literature report, there is similarity in the result. For example Sharma and Sharma, [19] reported that there is no association of abnormal creases with anomalies/diseases/ syndromes. There is also no association between altered brain morphology (as seen in schizophrenia) with altered dermatoglyphics features [13]. Contrary to our findings, the study of 95 Mexican epilepsy males, found quantitative significant differences between epileptic patients and normal individuals [27]. It was also reported that when comparing abnormal creases in Down's syndrome and normal subjects a higher total degree of transversatality (T-DoT) was found in Down's syndrome subjects. Similarly, a normal palmar creases of Down's syndrome show a higher T-DoT even when there is no specific abnormality in palmar creases (i.e. simian line or Sydney line and variants) [18]. This may supports the idea that quantitative analysis of the palmar creases may reveal more important variables for assessing the potential clinical significance of palmar creases in patients presented with congenital abnormalities (including epilepsy).
5. Conclusions
- In conclusion, the present study was able to demonstrate the prevalence of normal and abnormal creases in both epilepsy and control group. No significant association was found between palmar creases and epilepsy based on qualitative approaches of palmar analysis but yet significant association in the level of symmetry was observed in the study. This may support the idea of superiority of quantitative approaches over qualitative approaches in data analysis. Therefore, there may be a need of revisiting this study based on quantitative approach since the qualitative one fails to reveal significant association.
ACKNOWLEDGEMENTS
- The authors are grateful to the management of the Kumbotso Epilepsy Clinic for giving us the permission to carry out this research. Also appreciate the consent given by the participants and / or parents of the participants as well as those who contributed in the development of this research work.
References
| [1] | Berkovic, S.F, McIntosh, A., Howell, R., 1996. Familial temporal lobe epilepsy: A common disorder identified in twins Ann. Neurol. 40: 227-235. |
| [2] | Raymond, A.A., Fish, D.R., Sisodiya, S.M., 1995. Abnormalities of gyration, heterotopias, tuberous sclerosis, focal cortical dysplasia, microdysgenesis, dysembryoplastic neuroepithelial tumour and dysgenesis of the archicortex in epilepsy. Brain, 118: 629-660. |
| [3] | Palmini, A., Andermann, F., Olivier, A. 1991. Focal neuronal migration disorders and intractable epilepsy: a study of 30 patients. Ann. Neurol. 30, 741-749. |
| [4] | Steveson, R.E., Hane, B., Arena, J.F., May, M., Lawrence, L., Lubs, H.A., Schwartz, C.E., 1997. Arch finger prints, hypotonia and flexia associated with X linked mental retardation. J. Med. Genet. 34(6), 465-469. |
| [5] | Than, M. Myat, K. A, Khadijah, S., Jamaludin, N., Isa, M. U. 1998. Dermatoglyphics of Down’s syndrome patients in Malaysia, a comparative study. Anthropol. Anz. 56 (4), 351-365. |
| [6] | Schaumann, B., Alter, M. 1976. (eds). Dermatoglyphics in medical disorders, Springer Verlag, Berlin–Heidelberg–New York, 1–59. |
| [7] | Uchida, I. A., and Soltan, H. C., 1963. Evaluation of dermatoglyphics in medical genetics. Ped. Clin. N. Amer. 120, 409-422. |
| [8] | Penrose, L.S., 1963. Fingerprint, Palm and chromosomes, Nature 9, 933 – 8. |
| [9] | Jones, K.L., Robinson, L.K, Bakhireva, L.N. 2006. Accuracy of the diagnosis of physical features of fetal alcohol syndrome by pediatricians after specialized training, Pediatr. 118:1734-1738. |
| [10] | Cummins, H., Midlo, C., 1943. Finger prints, Palms and Soles Philadelphia: The Blakiston Company. |
| [11] | Babler, W., 1991. Embryologic development of epidermal ridges and their configurations In: Dermatoglyphics: Science in transition. Birth defects (Edited by: CC P, RM G, BA S) New York: Wiley-Liss, 95-112. |
| [12] | McGrath, J., Murray, R., 1995. Risk factors for Schizophrenia: from conception to birth In: Schizophrenia (Edited by: SR H, DR W) Victoria: Blackwell Science Ltd, 187-205. |
| [13] | Van Os, J., Woodruff, P., Fananas, L., Ahmed, F., Shuriquie, N., Howard, R., Murray, R., 2000. Association between cerebral structural abnormalities and dermatoglyphic ridge counts in schizophrenia. Compr. Psych. 41, 380-384. |
| [14] | Dar, H., Schmidt, R., Nitowsky, H.M., 1977. Palmar crease variants and their clinical significance: a study of newborns at risk. Pediatr. Res. 11(2), 103-8. |
| [15] | Chaube, R. 1977. Palmar creases in population studies. Am. J. Phys. Anthropol. 47, 7-9. |
| [16] | Park, J.S., Shin, D.S., Jung, W., Chung, M.S. 2010. Improved analysis of palm creases. Anat. Cell Biol., 43(2), 169-77. |
| [17] | Alter, M., 1970. Variation in palmar creases. Am. J. Dis. Child. 120, 424-431. |
| [18] | Dar, H., Schmidt, R., 1976. Topographic approach for analysis of palm crease variants. J. Med. Genet.13, 310-313. |
| [19] | Sharma, D. K., Sharma, V., 2010. Prevalence of Simian, Sydney and Suwon creases and their association with each other, body sides, handedness, gender and anomalies/ diseases/syndromes in a population of Central India. Int. J. Morphol. 29(3),1069-1075. |
| [20] | Lde Lestrange, M.T. 1969. The transverse crease in Europe: Index and comparative study of different samples cited in the literature. Am. J. Phys. Anthropol. 30(2), 173-82. |
| [21] | Oyinbo, C. A., Fawehinmi, H.B., 2009. Prevalence of Simian and Sydney creases in the Ijaws of South- South Nigeria. Int. J. Bio. Anthropol. 3(2), 2009. Avalaible in:prevalence-of-simianand-sydney-creases-in-the-ijaws-of-south-south-nigeria. |
| [22] | Adetona, M.O., Oladapo, O.O., Kinyemi, J.O., 2012. Palmar Flexion Creases Variants among Nigerians. Afr. J. Biomed. Res. 15, 93 – 96. |
| [23] | Hernández, M. 1985. Palmar creases in Spaniards. Anthropol. Anz. 43(2):187-90. |
| [24] | Rodrigues, L. 2009. Secrets of Hand Analysis. 2nd Ed., 2009. Avalaible in: http://handanalysis.com. |
| [25] | Blanka, S., Milton, A. 1976. Dermatoglyphics in Medical Disorders. Springer Verlag, New York-Heidelberg- Berlin, 1976: 253. |
| [26] | Ţarcă, A., Barabolski, C. 2002. Contributions to the dermatoglyphic diagnosis of epilepsy. J. Prev. Med. 10 (2), 28-34. |
| [27] | Labiano, L.M., 1989. Analysis of palmar creases in 95 Mexican epileptic males. Mendeliana, 9(1), 51-56. |