-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2014; 4(4): 105-107
doi:10.5923/j.ajmms.20140404.01
Long Term Cocaine Abuser Present with Systemic Sclerosis Like Symptom
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMaihemuti Axiyan, Benjamin Renelus, Khalid Bashir
Morehouse School of Medicine, Internal Medicine Department, Atlanta, Georgia, 30310, USA
Correspondence to: Maihemuti Axiyan, Morehouse School of Medicine, Internal Medicine Department, Atlanta, Georgia, 30310, USA.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
Background: Cocaine is one of the most commonly used illicit drugs in the United States. Systemic sclerosis is an autoimmune/connective tissue disease. Diagnosis based on clinical symptoms and positive serum markers. Case presentation: We present a case of an elder African American male with long history of cocaine abuse who presented with dry cough, dyspnea, dysphagia, skin tightness, and color changes. Conclusions: Systemic sclerosis is typically seen in young females with positive serum markers, but our patient, an older male with long history of cocaine abuse presented with classic systemic sclerosis like symptoms with negative serology. Long term Cocaine use can be present like systemic sclerosis like symptoms. It can be differentiated from autoimmune induced systemic sclerosis with positive serum markers. Treatment would be Symptomatic management with proton pump inhibitors and calcium channel blockers along with substance abuse cessation.
Keywords: Cocaine, Systemic Sclerosis, Long term
Cite this paper: Maihemuti Axiyan, Benjamin Renelus, Khalid Bashir, Long Term Cocaine Abuser Present with Systemic Sclerosis Like Symptom, American Journal of Medicine and Medical Sciences, Vol. 4 No. 4, 2014, pp. 105-107. doi: 10.5923/j.ajmms.20140404.01.
1. Introduction
- Cocaine is one of the most commonly used illicit drugs in the United States. Roughly 14% of the population aged 12 years and older, more than 30 million, have tried cocaine at least once [1].Systemic sclerosis is an autoimmune/connective tissue disease. Diagnosis based on clinical symptoms and positive serum markers. We present a case of an elder African American male with long history of cocaine abuse who presented with dry cough, dyspnea, dysphagia, skin tightness, and skin color changes.
2. Case
- 65 year old African American male with chronic obstructive pulmonary disease, hypertension, chronic polysubstance abuse (20+ years cigarettes, crack cocaine) presents with worsening dyspnea, cough, dysphagia. His dyspnea started about 4 years ago and has progressed over the year. He can barely walk across the room without resting and coughing. He also reported his fingers turning white in the cold for many years and had some digital ulcers that required amputation secondary to gangrene. Patient also reports skin thickness and tightening most notably in his hands. Long standing Gastroesophageal reflux disease, but more recent dysphagia for solids with “food stuck in throat feeling” prior to presentation. Work ups: White blood cell count with differentials within normal value. WBC=8.4, Hgb=11.6, Plt=234, Rheumatoid factor<20. Negative for Antinuclear antibodies, Anti-double strand DNA antibody, Anti-Jo-1antibody, anti-topoisomerase, Anti-Ribonucleoprotein Antibody, Anti-centromere antibody. Positive Urine toxic screening for cocaine. Heart Echocardiogram showed impairment of left ventricular relaxation. Patient was counseled regarding cocaine cessation. He was treated for symptomatic systemic sclerosis and given proton pump inhibitors for dyspepsia and calcium channel blockers for Raynaud’s. Patient was followed by Rheumatology while inpatient with expectant outpatient follow up accordingly.
 | Figure 1. Skin with salt and pepper changes, sclerodactyly status post amputation of 2nd, 3rd fingers. White spots on the chest wall |
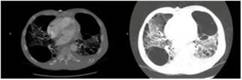 | Figure 2. Chest CT with Contrast: Extensive centrilobular emphysema with large biapical bulla, bibasilar reticular opacities with traction bronchiolectasis, Combined pulmonary fibrosis and emphysema |
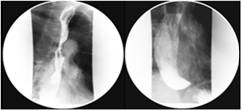 | Figure 3. Barium Swallow: Patulous and debris-filled esophagus with minimal peristalsis, can be seen in connective tissue disorders. Prominent cricopharyngeal achalasia |
3. Discussion
- Systemic sclerosis is a rare disease [2] with an annual incidence of 1 to 2 per 100,000 individuals in the United States. Etiology is unknown, Possible pathophysiology involves vascular intimal proliferation and fibrosis of visceral organs and dermis. Systemic sclerosis is classified by skin and visceral organ involvement which include limited cutaneous systemic sclerosis (lcSSc) and diffuse cutaneous systemic sclerosis (dcSSc). DcSSc is distinguished from lcSSc through proximal extremity and chest involvement along with involvement of visceral organs, including the kidneys, heart, lungs and in our case, the gastrointestinal tract. Diagnosis is made by clinical suspicion, presence of autoantibodies (specifically anti-centromere and anti-topoisomerase antibodies) and occasionally by biopsy. Of the antibodies, 90% have a detectable anti-nuclear antibody. Anti-centromere antibody is more common in the limited form (80-90%) than in the diffuse form (10%), and anti-topoisomerase is more common in the diffuse form (30-40%) and in African-American patients (who are more susceptible to the systemic form) [3]. There is no cure for scleroderma, and treatment is primarily symptomatic.Cocaine is one of the most commonly used illicit drugs in the United State over 4 million Americans reporting cocaine use within the year of 2012 [4]. The direct link between cocaine abuse and connective tissue disease has yet to be fully unearthed. Levamisole, an immunomodulating compound often used to lace/increase the potency of cocaine, has been postulated as the possible etiology of cocaine induced connective tissue disease. Levamisole was originally approved as an antihelminthic. It would subsequently be used for the treatment of autoimmune disorders such as nephrotic syndrome, rheumatoid arthritis and ultimately as an adjuvant to fluorouracil in the treatment of colon cancer [5]. Common adverse effect of levamisole include cutaneous vasculitis and agranulocytosis. Farmer [6] reported a case of full dermal thickness injury associated with presumed levamisole laced cocaine. The presumption that levamisole is the possible underlying etiology of connective tissue disease in cocaine users became a question of debate. In their case report of 3 cocaine abusing patients who was found to have serum positive connective tissue disease Sanchez-Cruz [7] suggest that levamisole was the source of the vasculopathy found in cases. Of note levamisole was not measured in these cases due to short half-life and limited available test for the drug. Sanchez-Cruz also found positive connective tissue serum markers for two of the cases reported including ANCA and ANA. Based on our knowledge of the literature there has been few cases of serum negative connective tissue disease in cocaine abusers. Clinicians should recognize the association and prevalence of connective tissue disease in cocaine abusers despite benign serology. Treatment of cocaine induced connective tissue disease is symptomatic with primary focus on cocaine cessation. Acid reducers with proton pump inhibitors are used dyspepsia secondary to esophageal dysmotility and calcium channel blockers are used for Raynaud’s phenomenon.
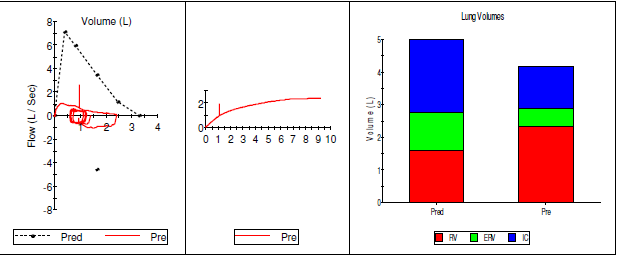 | Figure 4. Pulmonary Function Test: FEV1/FVC = 41%, FEV1 39%, DLCO corrected – 31 |
4. Conclusions
- Systemic sclerosis is typically seen in young females with positive serum markers, but our patient, an older male with long history of cocaine abuse presented with classic systemic sclerosis like symptoms with negative serology.Long term Cocaine use can be present like systemic sclerosis like symptoms. It can be differentiated from autoimmune induced systemic sclerosis with positive serum markers. Treatment would be Symptomatic management with proton pump inhibitors and calcium channel blockers along with substance abuse cessation. Treatment would be Symptomatic management with proton pump inhibitors and calcium channel blockers along with substance abuse cessation.
ACKNOWLEDGEMENTS
- We thank the patient for allowing us to share his details history and clinical presentation and thank for all the residents, attending physicians, nurses, laboratory technicians who involved in patient care.