-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2014; 4(2): 79-86
doi:10.5923/j.ajmms.20140402.09
The Impact of High Altitude on Endothelial Dysfunction of Cardiovascular Patients in Saudi Arabia: A Biochemical Study
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMohamed Abd Ellatif1, Abdullah S. Assiri2, Ayyub Patel1, Essam M. Nour Eldein3, Abdullah Al Marzouki4, Maha F. Hamoudah5, Zizi Saad6, Shirin H. Teama7, Waleed N. Hassan1
1Department of Clinical Biochemistry College of Medicine, King Khalid University, Abha, KSA
2Department of Internal Medicine, College of Medicine, King Khalid University, Abha, KSA
3Department of Clinical Chemistry, Faculty of Medicine, Umm Al-Qura University, Holy Makkah, KSA
4Department of Internal Medicine, Faculty of Medicine, Umm Al-Qura University, Holy Makkah, KSA
5Department of Clinical Chemistry Aseer Central Hospital, Abha, KSA
6Department of Cardiology, Aseer Central Hospital, Abha, KSA
7Department of Clinical Chemistry, King Abdulaziz Hospital, Holy Makkah, KSA
Correspondence to: Mohamed Abd Ellatif, Department of Clinical Biochemistry College of Medicine, King Khalid University, Abha, KSA.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
High-altitude dwellers have successfully evolved adaptive regulatory mechanisms to survive in a chronic hypoxic environment. Risk assessment regarding high altitude exposure of patients with coronary heart disease (CHD) is of increasing interest. The aim of our study, therefore, was to investigate the biochemical effect of high altitude on modulation of the adaptive response of endothelial functions in patients with cardiovascular diseases (CVD) including myocardial ischemia (MI) or CHD patients living at high altitudein Saudi Arabia. Subjects: This study included 271 subjects composed of 136 patients (84 men and 52 women) suffering from cardiovascular diseases with age range 40 - 68 (mean 54) years, and 135 apparently healthy control subjects (69 men and 66 women) with age range 40 - 65 (mean 52.5) years. All individuals selected for this study were divided into four groups: A- 68 patients suffering from CVD from the cardiology outpatient clinic of Aseer Central Hospital, Abha city, KSA (2,200 meters above sea level) representing high altitude group. B- 68 apparently healthy control volunteer subjects from Abha city, KSA. C- 68 patients suffering from CVD from the cardiology outpatient clinic of King Abdulaziz Hospital, Makkah city, representing sea level group. D- 67 apparently healthy control volunteer subjects from Makkah city. Methods: Serum biochemical measurements for patients and healthy subjects were performed including: Fasting blood sugar, kidney and liver function tests, plasma lipid profile including: total cholesterol (TC), High density lipoprotein cholesterol (HDLc), Low Density Lipoprotein (LDLc) and triglycerides (TG). In addition, parameters of vascular endothelial functions including: Nitric Oxide (NO) in the form of serum nitrite and nitrate (NO2-/NO3-) concentrations, serum endothelin-1 (ET-1) and vascular cell adhesion molecule (VCAM-1) were also measured. Results: Measurements confirmed higher levels of ET-1 in high altitude control healthy subjects compared with those at sea level (P < 0.001) and also in high altitude cardiovascular patients compared with those at sea level (P < 0.001). Our results also, showed that there was a significant elevation of serum levels of ET-1 in patients group compared to the healthy control group either at high altitude (P < 0.001) or at sea level (P < 0.001). As regards VCAM-1, our results confirmed higher serum levels of VCAM-1 in high altitude control healthy subjects compared with those at sea level (P = 0.015) and also in high altitude cardiovascular patients compared with those at sea level (P = 0.013). Our results also, showed that, there are was a significant elevation of serum levels of VCAM-1 in patients group compared to the healthy control group either at high altitude (P < 0.001) or at sea level (P < 0.001). Our results confirmed higher levels of nitrite/nitrate in high altitude control healthy subjects compared with those at sea level (P = 0.003) and also in high altitude cardiovascular patients compared with those at sea level (P = 0.01). In conclusion,our data suggest that chronic hypoxia at high altitude may lead to higher circulating concentrations of these important vasoactive compounds (VCAM-1, ET-1 and NO), either as a direct result of hypoxia or as adaptive response to chronic high-altitude exposure. This process could imply a potential role for the measurement of these compounds in the prognostic evaluation of patients with CVD. Future studies with the use of ET receptor antagonists as part of a multidrug regimen are also needed especially for cardiovascular disease patients living at high altitude.
Keywords: Endothelin-1, VCAM-1, Nitric Oxide, High altitude, Endothelial Dysfunction
Cite this paper: Mohamed Abd Ellatif, Abdullah S. Assiri, Ayyub Patel, Essam M. Nour Eldein, Abdullah Al Marzouki, Maha F. Hamoudah, Zizi Saad, Shirin H. Teama, Waleed N. Hassan, The Impact of High Altitude on Endothelial Dysfunction of Cardiovascular Patients in Saudi Arabia: A Biochemical Study, American Journal of Medicine and Medical Sciences, Vol. 4 No. 2, 2014, pp. 79-86. doi: 10.5923/j.ajmms.20140402.09.
Article Outline
1. Introduction
- The healthy endothelium is a dynamic organ that regulates vascular tone by balancing production of vasodilators and vasoconstrictors in response to a variety of stimuli [1]. The endothelium, senses mechanical stimuli, such as pressure stress, and hormonal stimuli, such as vasoactive substances. In response, it releases agents that regulate vasomotor function, trigger inflammatory processes, and affect hemostasis [2]. Endothelial dysfunction can be defined as an imbalance between vaso-dilating and vaso-constricting substances [3]. Vascular endothelial dysfunction is observed in several forms of cardiovascular diseases (CVD) [2, 4], and it is also associated with CVD risk factors e.g. smoking, hypertension, and obesity [5-7]. Changes in endothelium function may lead to the coronary artery circulation being unable to cope with the increased metabolism of myocardial muscle independently of a reduced coronary artery diameter [8]. Given its central role in the development of coronary and peripheral artery diseases, vascular endothelial dysfunction is considered an important target for reducing the risk of CVD morbidity and mortality [4].Cell adhesion molecules have been implicated in many pathological processes such as inflammation, wound healing and atherosclerosis. Vascular cell adhesion molecules -1 (VCAM-1) is expressed on activated endothelium, and is involved in leukocyte attachment and transmigration [9]. Endothelial dysfunction is associated with arterial inflammation, that makes the cell adhesion markers such as intercellular adhesion molecule-1 (ICAM-1), VCAM-1, and E-selectin, of a great value as diagnostic and prognostic markers, or as potential targets for therapeutic intervention [2,10]. Endothelin-1 (ET-1) is a potent vasoconstrictor peptide produced locally by the vascular endothelium and modulates vascular smooth muscle cell proliferation [11-13]. ET-1 is implicated in the pathophysiology of CVD and it has been suggested as a potential marker of endothelial dysfunction [2, 14, 15].Nitric oxide (NO) is a potent endogenous vasodilator synthesized from L-arginine by a family of NO synthases [16-18]. NO is implicated in many physiological functions e.g. immune response, synaptic transmission and dilation of blood vessels. Also, NO is a signaling molecule for the control of blood pressure, and blood flow [19] and it is an important antioxidant [20]. NO is the predominant mediator of normal vascular function, causing smooth muscle relaxation in response to stimulation by other factors such as ischemia [1], so NO availability is an important diagnostic and prognostic factor. The plasma level of total NO, i.e., the sum of nitrite (NO2−) and nitrate (NO3−), is frequently used to assess NO availability in vivo [21]. Endothelial dysfunction is characterized by reduced endothelial NO synthase activity, attenuated NO release, or increased NO degradation [22].High altitude exposure triggers physiologic responses for maintaining an adequate tissue oxygenation [23]. Subjects who adapted to these altitudes for many months or years may develop chronic mountain sickness (CMS), which is characterized by excessive production of red cells, hypoventilation, fatigue, dyspnea, cyanosis, clubbing of the fingers and leg edema [24]. High altitude induces changes in cardiac rhythm that may explain the higher rate of sudden cardiac death at high altitude. This, in addition to the respiratory alkalosis, may further predispose to palpitations, arrhythmias and ischemia, especially in those with pre-existing cardiac disease [25]. Coronary spasm may be induced by sympathetic activation and alkalosis. Nevertheless, at 2000 to 2500 m above sea level, mild hypoxemia is induced, alkalosis is minor [26]. In CMS occurring in long-life residents living above 2,500 metres, excessive erythrocytosis coupled with hypoxic pulmonary vaso-constriction may result in high pulmonary artery pressures, leading to congestive heart failure [27]. Defense mechanisms include erythropoiesis and angiogenesis to augment red blood cell mass and oxygen delivery, and increases utilization of oxygen-efficient fuel substrates such as carbohydrates [28]. High altitude residents have adaptive mechanisms to survive in such hypoxic environment [15]. These adaptive mechanisms, although generally tolerated by most healthy subjects, may induce major problems in patients with preexisting CVD [23]. Exposure to high altitude may unmask coronary artery disease, left ventricular dysfunction, or pulmonary hypertension that was asymptomatic at sea level [26]. For patients with CVD, the high-altitude environment poses some physiological challenges than normal subjects [29]. The knowledge about the molecular mechanisms and related intracellular signaling pathways, and pharmacological treatment options regarding endothelial dysfunction at high altitude is still accumulating [22].The aim of our study was to investigate the biochemical effect of high altitude on modulation of the adaptive response of endothelial functions in patients with CVD living at high altitude in Saudi Arabia.
2. Subjects and Methods
2.1. Subjects
- This study included 271 subjects composed of 136 patients (84 male and 52 female) suffering from CVD including MI or CHD patients with age range 40 – 68 (mean 54) years, and 135 apparently healthy control subjects (69 male and 66 female) with age range 40 – 65 (mean 52.5) years.Exclusion criteria: Smoking, history and clinical signs of heart failure, hyperlipidemia, autoimmune disease, or any other chronic illness, such as cancer, chronic liver disease, and chronic renal disease. Also, subjects with any infections, acute or chronic inflammatory disease, and patients with neural complications. All individuals selected for this study were living in the same area for the last five years and they were divided into four groups: A- 68 patients suffering from CVD from the cardiology outpatient clinic of Aseer Central Hospital, Abha city, KSA (2,200 meters above sea level) representing high altitude group. B- 68 apparently healthy control volunteer subjects from Abha city, KSA. C- 68 patients suffering from CVD from the cardiology outpatient clinic of King Abdulaziz Hospital, Makkah city, representing sea level group. D- 67 apparently healthy control volunteer subjects from Makkah city. In terms of other known conditions associated with endothelial dysfunction (arterial hypertension or diabetes mellitus), the groups of patients were matched. All patients and control subjects were subjected to a thorough history taking and general medical examination. ECG and Echocardiography were performed for the assessment of patients included for the study. Written informed consent was obtained from all patients and healthy volunteers according to the declaration of Helsinki and the study was approved by the Ethics Committee of College of Medicine, King Khalid University.
2.2. Blood Sampling
- Fasting venous peripheral blood samples (10 ml) were obtained from all subjects. Blood samples were drawn into plain tubes. The blood was centrifuged and the serum was separated into 0.5 ml aliquots and frozen at - 80°C for subsequent analysis. Several serum biochemical measurements for patients and healthy subjects were made which include Routine chemical analysis including: Fasting blood sugar, kidney and liver function tests, plasma lipid profile including: total cholesterol (TC), High density lipoprotein cholesterol (HDLc), Low Density Lipoprotein (LDLc) and Triacylglycerol (TAG). Parameters of vascular endothelial functions including: NO in the form of serum nitrite and nitrate concentrations, ET-1 and VCAM-1 were also measured.
2.3. Methods
- The biochemical parameters including kidney function tests, liver function tests and lipid profile were determined using commercial reagents with an automated chemical analyzer (Abbott analyzer, Abbott Laboratories, Abbott Park, Chicago, IL).1. Measurement of the serum endothelin-1 (ET-1) was performed by human endothelin-1 immunoassay kit (Cayman chemical, Ann Arbor, MI, USA) using monoclonal antibody specific for endothelin. The concentration is determined by measuring the enzymatic activity of acetylcholine estrase at 412 nm against the standard curve using the plate reader (Human, Wiesbaden, Germany). The intra-assay coefficient of variation was 4.4% and the inter-assay coefficient of variation was 5.2% [30].2. Serum level of VCAM-1 was assessed by commercial ELISA: Human sVCAM-1 ELISA kit (Abnova, Jhongli, Taiwan), following the manufacturers’ instructions. ELISA experiments were run simultaneously on all samples. The test is using Biotin / Avidin conjugate and the absorbance is measured at 450 nm using the plate reader (Human, Wiesbaden, Germany). The sensitivity of the test was determined to be 0.6 ng/ml. The intra-assay coefficient of variation was 3.1% and the inter-assay coefficient of variation was 5.2%.3. For total nitrite / nitrate measurement we used colorimetric assay kit (Cayman chemical, Ann Arbor, MI, USA). The serum samples were first thawed, then de-proteinized by adding zinc sulfate. Deproteinization is a necessary step in the measurement of serum nitrite concentrations [31]. The deproteinized serum (100 μL) was applied in duplicate to a 96-well ELISA plate, 100 μL of vanadium (III) chloride (8 mg/mL) was added to each well (for reduction of nitrate to nitrite) followed by the addition of 100 μL of Griess reagent (equal mixture of 1% sulphanilamide in 5% phosphoric acid and 0.1% N-(1-naphthyl) ethylenediamine hydrochloride in distilled water). The plates were incubated for 30 minutes at RT and the optical density was measured at 540 nm using the plate reader (Human, Wiesbaden, Germany). A two-fold dilution series (0.193 - 100 μM) of NaNO2 was prepared from 100 μM NaNO2 solution using distilled water. Each dilution (100 μL) was mixed with an equal volume of Griess reagent, and the optical density was measured at 540 nm. A standard curve was plotted. The intra-assay coefficient of variation was 3.4% and the inter-assay coefficient of variation was 2.7% [32].
2.4. Statistical Analysis of Final Results
- The data were statistically analyzed using the Statistical Package for the Social Sciences software (SPSS version 13.0). The data were categorized as parametric and showed preserved normality, using kolmogrov-Smirnov test, and were presented as mean ± standard error of mean (SEM). The independent sample t - test was applied for analysis of difference between each two groups. A probability (P value) of 0.05 was considered to be statistically significant.
3. Results
3.1. Lipid Profile
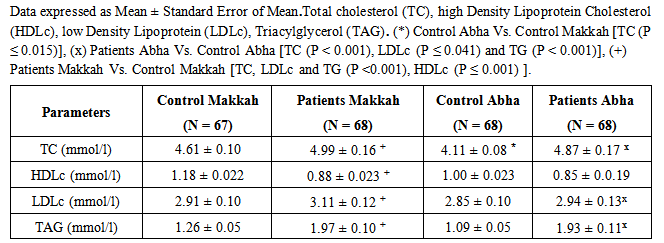
- The data presented in table (1) showed that the high altitude control subjects had average total cholesterol of 4.11 mmol/l, HDLc 1.00 mmol/l, LDLc 2.85 mmol/l and TAG 1.09 mmol/l while patients had average total cholesterol of 4.87 mmol/l, HDLc 0.85 mmol/l, LDLc 2.94 mmol/l and TAG 1.93 mmol/l. Sea level control had average total cholesterol of 4.61 mmol/l, HDLc 1.18 mmol/l, LDLc 2.91 mmol/l and TAG of 1.26 mmol/l while patients had average total cholesterol of 4.99 mmol/l , HDLc 0.88 mmol/l, LDLc 3.11 mmol/l and TAG of 1.97 mmol/l. Measurements confirmed significant higher levels of total cholesterol (P < 0.001), LDLc (P < 0.001) and TAG (P < 0.001) with significant lower levels of LDLc (P ≤ 0.041) in high altitude patients compared with healthy control subjects in high altitude. Also, there were significant higher levels of total cholesterol (P < 0.001), LDLc (P < 0.001) and TAG (P < 0.001) with significant low HDLc (P ≤ 0.001) in sea level patients compared with healthy control subjects at the same level. Our results also, showed non-significant differences of lipid profile levels between subjects of high altitude and sea level either patients or control, except the higher serum level of total cholesterol in healthy individuals of sea level high altitude compared to those of high altitude (P ≤ 0.015).
|
3.2. ET-1
- The high altitude control and patients had average ET-1 serum levels of 2.30 ± 0.02 pg/ml and 3.31 ± 0.24 pg/ml, respectively, whereas sea level control and patients had average serum nitrite/nitrate of 1.99 ± 0.05 pg/ml and 2.84 ± 0.12 pg/ml, respectively (Fig.1). Measurements confirmed higher levels of ET-1 in high altitude control healthy subjects compared with those at sea level (P < 0.001) and also in high altitude cardiovascular patients compared with those at sea level (P < 0.001). Our results also, showed that, there is a significant elevation of serum levels of ET-1 in patients group compared to the healthy control group either at high altitude (P < 0.001) or at sea level (P < 0.001).
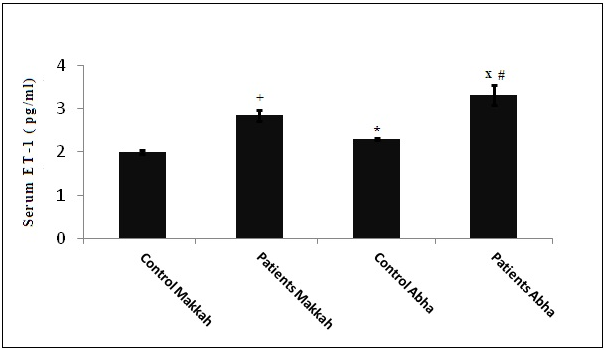 | Figure 1. Serum Endothelin-1 (ET-1) levels in different groups: (*) Control Abha Vs. Control Makkah P < 0.001, (x) Patients Abha Vs. Control Abha P < 0.001, (#) Patients Abha Vs Patients Makkah P < 0.001, (+) Patients Makkah Vs. Control Makkah P < 0.001 |
3.3. VCAM-1
- The high altitude control and patients had average VCAM-1 serum levels of 1261.3 ± 31.6 ng/ml and 1491.2 ± 59.4 ng/ml, respectively, whereas sea level control and patients had average serum VCAM-1 of 1043.8±21.6 ng/ml and 1276.0±38.9ng/ml, respectively (Fig. 2). Measurements confirmed higher serum levels of VCAM-1 in high altitude control healthy subjects compared with those at sea level (P ≤ 0.015) and also in high altitude cardiovascular patients compared with those at sea level (P ≤ 0.013). Our results also, showed that, there is a significant elevation of serum levels of VCAM-1 in patients group compared to the healthy control group either at high altitude (P < 0.001) or at sea level (P < 0.001).
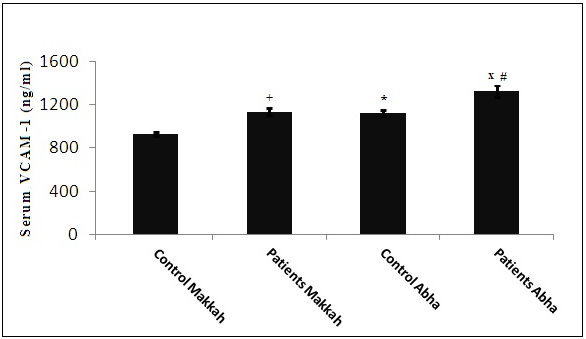 | Figure 2. Serum vascular cell adhesion molecule-1 levels in different groups: (*) Control Abha Vs. Control Makkah P = 0.015, (x) Patients Abha Vs. Control Abha P < 0.001, (#) Patients Abha Vs Patients Makkah P ≤ 0.013, (+) Patients Makkah Vs. Control Makkah P < 0.001 |
3.4. Nitrite/Nitrate
- The high altitude control and patients had average serum level of nitrate/nitrite of 120.1 ± 2.5 nmol/ml and 125.6 ± 3.1 nmol/ml, respectively, whereas sea level control and patients had average serum nitrite/nitrate of 106.5 ± 1.5 nmol/ml and 116.6 ± 3.1 nmol/ml, respectively (Fig. 3). Measurements confirmed higher levels of nitrite/nitrate in high altitude control healthy subjects compared with those at sea level (P ≤ 0.003) and also in high altitude cardiovascular patients compared with those at sea level (P ≤ 0.01).
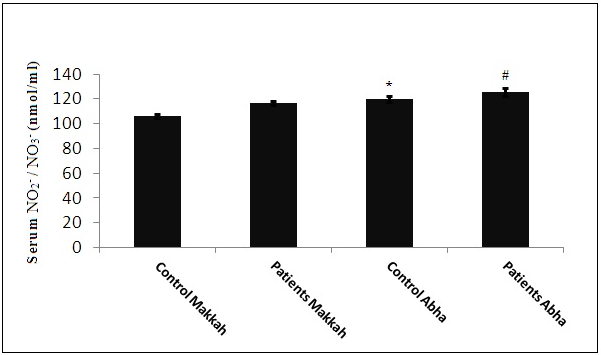 | Figure 3. Serum Nitrite/Nitrate (NO2- / NO3- ) levels in different groups: (*) Control Abha Vs. Control Makkah, P ≤ 0.015, (#) Patients Abha Vs Patients Makkah P ≤ 0.013 |
4. Discussion
- To the best of our knowledge, this is the first biochemical study to directly investigate the impact of high altitude on endothelial dysfunctions in human CVD in Saudi Arabia. At high-altitude, differences in barometric pressure result in hypoxia which is subject to adaptation [33]. Circulating endothelial markers have been proposed as potential alternatives for evaluation of the endothelium in condition of vascular disorders [34]. Endothelin-1 is a potent endogenous vasoconstrictor whereas NO is a vasodilator [17]. The interactions among various biomarkers remained unexplored under the stressful environment of high-altitude [35]. Our study showed higher levels of ET-1 in high altitude control healthy subjects compared with those at sea level (P < 0.001) and also in high altitude cardiovascular patients compared with those at sea level (P < 0.001). These findings support the previous results that hypoxia leads to higher ET-1 levels and contributes to the increased hypoxic vasoconstriction [36-38]. In the Mount Everest study it has been observed that at high altitude an increase of plasma ET-1 compared to values found at sea level. These changes tended to decrease rapidly with the return to lower altitudes [39]. The elevated level of ET-1 in high altitude subjects (patients and healthy control) could be explained by the up-regulation of ET-1 gene expression by hypoxia which, also, stimulates the induction of genes encoding growth factors for blood vessels and remodeling enzymes [40]. Our results also, showed that, there is a significant elevation of serum levels of ET-1 in cardiovascular patients compared to the healthy control either at high altitude (P < 0.001) or at sea level (P < 0.001). These findings are quite consistent with previous studies that plasma ET-1 levels are elevated in patients with symptomatic atherosclerosis, heart failure and primary pulmonary hypertension [2]. In our study, cardiovascular patients had abnormal lipid profile compared to healthy controls, which may share in stimulation of ET- production which could be stimulated by LDL-c and high-cholesterol. Oxidized LDL-c induces the production of ET-1 in human macrophages and increases ET-1 release from endothelial cells [41, 42]. Because of the effects of ET-1 in promoting vasoconstriction, smooth muscle cell proliferation, neutrophil adhesion, and platelet aggregation, this likely contributes to CVD [42]. The dysfunctional endothelium contributes to increased vascular stiffness, impairs myocardial perfusion, and worsens ventricular function [43, 44]. Because of the potent vaso-constricting effects of ET-1 and its involvement in various CVD, blockade of the ET-1 receptor has received considerable attention [17, 42]. ET-1 antagonists are promising new agents in the treatment of cardiovascular diseases [12, 45]. Also, ET-1 production can be inhibited through renin-angiotensin system inhibitors or statins, which reduce ET-1 expression independently of their lipid-lowering effects [45].Endothelial dysfunction is also characterized by increased production of endothelium-derived contracting factors, including angiotensin II and prostanoids [22] which will lead to increase in systemic blood pressure especially with significant changes at 1200 to 3000 m above sea level [29]. This leads to cell growth and inflammation by the activation of nuclear factor-κB (NF-κB), vascular cell adhesion molecule (VCAM) and interleukin-6 (IL-6). VCAM and cytokine action increases the adhesiveness of the endothelium and subsequently the binding of inflammatory cells to the endothelial surface leading to vascular inflammation and thrombosis [3]. Our study showed higher levels of serum VCAM-1 in high altitude control subjects compared to those at sea level (P ≤ 0.015). Also, cardiovascular patients in high altitude had higher levels of serum VCAM-1 compared with those at sea level (P ≤ 0.013). The elevated serum VCAM-1 levels in high altitude residents could be explained by the up regulation of VCAM-1 gene. It is known that the hypoxic inducible factor-1 (HIF-1) is involved in the up regulation of several genes including VCAM-1 [38]. Our results also, showed that, there is a significant elevation of serum levels of VCAM-1 in patients group compared to the healthy control group either at high altitude (P < 0.001) or at sea level (P < 0.001). These results are quite consistent with previous studies which revealed that VCAM-1 is one of the independent risk factors for cardiovascular diseases. Clinical studies have shown that elevated serum concentrations of cell adhesion molecules such as VCAM-1 may be independent risk factors for atherosclerosis and CVD [46, 47]. In our study, NO blood levels, estimated by measuring its stable metabolites, nitrite (NO2-) and nitrate (NO3-), were higher in high altitude control healthy subjects compared with those at sea level (P ≤ 0.003) and also in high altitude cardiovascular patients compared with those at sea level (P ≤ 0.01). Cultured endothelial cells have shown an increased production of NO, expression of endothelial NO synthase under hypoxia at the transcriptional level [48-50]. Our findings are consistent with other observations of elevated NO metabolite concentrations in the blood of highlanders [12, 13, 51]. Activation of NO system in high altitude is a probable adaptive mechanism of cardio-vascular system to hypoxia and micro-vascular blood flow. Such increased NO stable metabolites blood level in high altitude residents may explain the vaso-dilative reserve and strengthening of cardiac pump and contractile functions for adequate tissue perfusion and optimal oxygen supply [52, 53]. Recent reports support the notion that high nitrite/nitrate levels in high altitude residents might be an integral part of the human physiological response to hypoxia [54, 55]. Increased longer-lived NO metabolites such as nitrite and nitrate levels were associated with changes in microcirculatory blood flow which may affect local tissue oxygen delivery through cGMP-independent mechanism [51]. Our study is limited regarding the changes in NO metabolite levels in vascular tissue, skeletal muscle, or red blood cells, which also expected to contribute to the physiological adaptations. Moreover, it remains unclear whether NO itself or a change in NO-related post-translational modification of proteins or transcription factors, may contribute to beneficial adaptation to hypoxia. Although the main objective of our study was to assess the quantitative changes of the NO metabolites in high altitude, several biochemical parameters variables are worthy of further investigation. Our results suggest that NO is an integral part of the human physiological response to hypoxia. These findings may be of relevance not only to healthy subjects exposed to high altitude but also to patients in whom oxygen availability is limited through disease affecting the heart, lung or vasculature [52].
5. Conclusions
- In conclusion, our data suggest that chronic hypoxia at high altitude may lead to higher circulating concentrations of these important vasoactive compounds (VCAM-1, ET-1 and NO), either as a direct result of hypoxia or as adaptive response to chronic high-altitude exposure. This process could imply a potential role for the measurement of these compounds in the prognostic evaluation of patients with CVD. Future studies with the use of ET receptor antagonists as part of a multidrug regimen are also needed especially for cardiovascular disease patients living at high altitude.
ACKNOWLEDGEMENTS
- This research was fully supported by a grant from the Deanship of Scientific Research, King Khalid University, Abha, Kingdom of Saudi Arabia.
Conflict of Interest
- Authors received no financial support from any industry to conduct this study, and no conflicts of interest in performing this study that might bias the interpretation of results.