-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2014; 4(2): 72-78
doi:10.5923/j.ajmms.20140402.08
Infection Associated Hemophagocytic Histiocytosis and Its Effect on Hematological Parameters
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLWaseem Iqbal 1, Muhammad Raza 2, Faisal Mughal 3
1Department of Pathology, College of Medicine, Qassim University, Buraidah 51452, Qassim - Saudi Arabia
2Department of Pharmacology and Therapeutics, College of Medicine, Qassim University, Buraidah 51452, Qassim - Saudi Arabia
3Department of Anatomy and Histology, College of Medicine, Qassim University, Buraidah 51452, Qassim - Saudi Arabia
Correspondence to: Waseem Iqbal , Department of Pathology, College of Medicine, Qassim University, Buraidah 51452, Qassim - Saudi Arabia.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
Infection associated hemophagocytosis may result from immunologic activation of mononuclear phagocyte system. The phenomenon of HP may affect various organ functions and hematological parameters. Exaggerated HP can lead to HPS which is a fatal condition. Recognizing and treating this disorder (anticytokine therapy) and underlying infection may save the life of the patient. The aim of the present study was to determine the etiology and grading of hemophagocytosis (HP) associated with infection and its effect on haematological parameters, and, to correlate it with the clinicopathological effects of hemophagocytic syndrome (HPS). A total of sixty two patients suffering from infection of varied etiology were included in this study. Bone marrow aspiration was done in all the cases along with complete blood counts. Bone marrow smears were examined for HP and its intensity and effect on hematological parameters was recorded. Among the sixty two patients included in this study, 27% (17/62) had viral infection followed by enteric fever (21%; 13/62), tuberculosis and visceral leishmaniasis (14% each; 9/62 each), malaria (13%; 8/62), brucellosis and others (5% each; 3/62). Most patients showed either moderate (grade II, 50%; 31/62) or severe degree (grade III, 34%; 21/62) of HP. Hemophagocytic syndrome was present in 34% patients. Patients with increased intensity of HP in the bone marrow had profound effect on hematological parameters; particularly hemoglobin and platelet count, resulting in the depression of these formed elements. Viral, bacterial and parasitic infections play an important role in the causation of histiocytic hyperplasia with HP. It may present as HPS with multisystem disorder which could be fatal if improperly diagnosed and left untreated. Severe intensity of HP has a profound effect on hematology parameters of patients particularly on hemoglobin level, total leukocyte count) and platelet count with a drastic decrease in all of the parameters during the severe disease course.
Keywords: Hemophagocytosis, Hemophagocytic Syndrome, Grading and Severity
Cite this paper: Waseem Iqbal , Muhammad Raza , Faisal Mughal , Infection Associated Hemophagocytic Histiocytosis and Its Effect on Hematological Parameters, American Journal of Medicine and Medical Sciences, Vol. 4 No. 2, 2014, pp. 72-78. doi: 10.5923/j.ajmms.20140402.08.
Article Outline
1. Introduction
- Hemophagocytosis (HP) has been reported in the literature under various diagnostic terms like histiocytic medullary reticulosis, malignant histiocytosis or infection associated hemophagocytosis [1] and is described to result from immunologic activation of the mononuclear phagocytic system (reactive), neoplastic proliferation of histiocytes (malignant) and a genetic or chromosomal derangement [2]. In reactive histiocytosis which is mainly associated with infection the macrophages are mature in contrast to malignant histiocytosis that demonstrates mainly immature proliferating cells. The mature macrophages are characterized by low nuclear cytoplasmic ratio, condensed chromatin pattern, inconspicuous nucleoli and abundant cytoplasm. Hemophgocytosis with histiocytic hyperplasia may present as hemophagocytic syndrome (HPS) [3]. This clinicopathologic entity is characterized by increased proliferation and activation of macrophages and T-lymphocytes with hemophagocytosis. Risdall et al., [4] ascribed it to the viral infection. Clinical features and biochemical events of HPS include fever of unknown etiology, cytopenias, hepatosplenomegaly, coagulopathy, hyperferritinemia, liver dysfunction and derangement in lipid metabolism. It may be primary as observed in familial hemophagocytic lymphohistiocytosis (FHL), X-linked lymphoproliferative syndrome (XLP), Chédiak–Higashi syndrome (CHS) and Griscelli syndrome (GS), or secondary to infection, malignancy, autoimmune disease, drugs, non-malignant hematological conditions and a variety of other diverse disorders [2, 5]. Clinical features and their biological manifestation in both infection associated and non-infection associated cases, result from hypercytokinemia by activated T-cells and macrophages [6]. Patients with active HPS demonstrate serum levels of Th1 cytokine IFN-γ, Interleukin (IL)-12 and IL-18 significantly higher than in the remission phase of the disease or in healthy controls. IL-18 seems to play a pivotal role in inducing IFN-γ and IL-12 and it has been found to be particularly elevated in tuberculosis and autoimmune disorders. Serum levels of proinflammtory cytokines TNF-α, IL-1B and IL-6 also, remain elevated in patients with active HPS in comparison to controls, whereas this appears at variance in the case with Th2 cytokine IL-4 [7]. Serum levels of both IL-1 and IL-10 appear elevated in patients with active HPS. However, the amount of IL-10 produced remains insufficient to influence Th1 cytokine production [1].
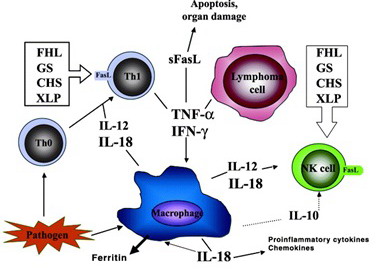 | Figure 1. Shows the proposed pathophysiology of HPS [2] |
2. Materials and Methods
2.1. Histopathological Procedure
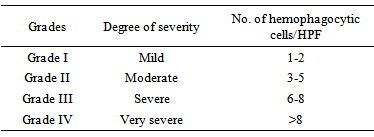
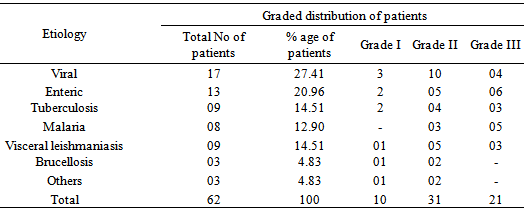
- A total of sixty two patients having different underlying infections (viral, bacterial and parasitic) were included in the study. A detailed history was taken and a complete physical examination was done in each patient. In the light of history, physical examination, blood and bone marrow findings, Widal test, viral screening, culture for microbes and serological tests were carried out in relevant cases to establish the cause of infection. Patients with established cause were selected to be included in this study. Bone marrow aspiration was done in all the patients and trephine biopsy was carried out in the relevant subjects at Pakistan Institute of Medical Sciences and Riphah University allied teaching hospitals Islamabad, Pakistan. The period of study spanned between March 2009 and March 2011. The ethical procedures outlined in the regulation procedures of both the institutions were followed.A standardized technique was used to obtain bone marrow aspirate and smear preparation [18]. All the Leishman stained bone marrow aspiration smears were examined for hemophagocytosis; and grading for the intensity of this phenomenon was also carried out. Complete blood counts, reticulocyte count, absolute values and RBC morphology were performed in each subject. For cell counts and absolute value hematology analyzer Sysmex® K1000 was used. Liver function tests, coagulation studies, lipid profile and, serum ferritin levels were also determined in certain patients to establish the presence or absence of hemophagocytic syndrome. These fixed slides were stained with Leishman stain (Sigma Geigy stain catalogue No. 3742) using the routine standardized procedure [18]. The slides were examined under the microscope using low power as well as high power (high dry and oil immersion) for pathomorphological changes such as cellularity of bone marrow in general, cellularity and maturation of erythropoiesis, myelopoiesis and megakaryocytes. The smears were also examined for lymphocytes, abnormal cells, histiocytes, hemophagocytosis and parasites. Grading of intensity of HP was done on bone marrow aspiration smears in order to determine the severity of this phenomenon. The mounted slides were first scanned under low power (X10) in 10 random fields and presence or absence of HP was tabulated. Slides were then examined under high power (high, X40) to grade the intensity of HP. The number of phagocytic cells was counted in 10 random fields and average of such cells per high power field (HPF) was calculated and used in grading the phenomenon of HP. The intensity of HP was graded depending upon the number of hemophagocytic cells per high power field using an arbitrary scale given in the Table 1.
|
2.2. Microbiological Test Procedures
- At the time of bone marrow aspiration, 2ml of aspirated material was mixed with brain heart infusion (BHI medium) for routine culture in relevant cases. Löwenstein–Jensen medium was used for acid fast bacilli (AFB) and inoculated with 0.5 ml of bone marrow aspirate. The culture bottles were then subject to the culture and sensitivity testing.
2.3. Statistical Analysis
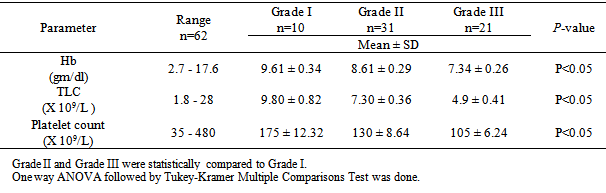
- GraphPad InStat® 3.10, version 1.3.2 was employed for statistical inference. Data are presented as direct numbers or expressed as percentage of the total. Data in table 3 are expressed as mean ± SD. The one way analysis of variance (ANOVA) followed by Tukey-Kramer multiple comparisons test was done. P<0.05 is considered to be statistically significant. The results on the severity of the pathomorphological findings were expressed according to an arbitrary scale (high power field; HPF) in each case and were compared with observations in grade I.
3. Results
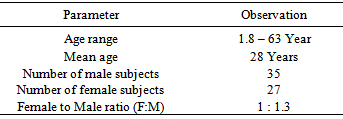
- The age of the HP patients ranged from 1.8 years to 63 years and female to male ratio of 1:1.3 (Table 2). Fever was the most common symptom at the time of presentation, occurring in all cases (100%). This was followed by cough (63%), generalized weakness (58%), diarrhoea, bleeding and night sweats. Sixty two patients with different underlying infections showing HP in the bone marrow were included in the study (Table 3).
|
|

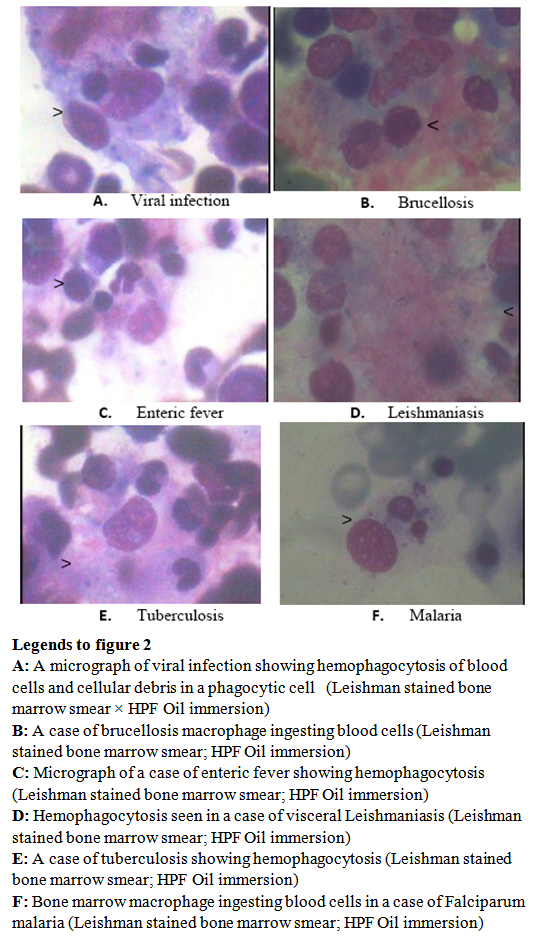 | Figure 2. Micrographs showing phenomena of HP in infections due to various etiologies pointed to by the arrow heads (>) |
|
|
|
4. Discussion
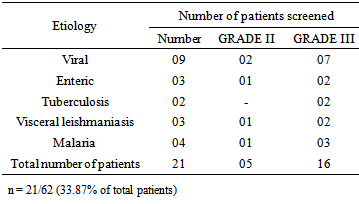
- In the present study variable degrees of hemophagocytosis were observed in 62 patients subjected to bone marrow examination having different underlying infections. Scott and Robb-Smith [19] described it as histiocytic medullary reticulosis and it was invariably believed to be neoplastic. In the present study, 17 patients with viral infection showed variable intensity of HP. Risdall et al., [4] studied 19 patients with active viral infection. The bone marrow smears in those cases showed histiocytic hyperplasia with prominent HP. Most of those patients presented as hemophagocytic syndrome. Apart from the study of Risdall et al., [4] other workers have also isolated different viral agents including Herpes simplex , Epstein Barr virus [17], CMV [20], HIV [21] and Parvovirus B19 [22] as a cause of virus associated HPS. Ohga et al., [11] studied the role of T-cell in chronic active EBV infection. EBV and cytokine gene expression was quantified by the use of PCR among 6 patients. Fractionated CD3+HLA-DR+ cells from patients with chronic active EBV infection contained higher copies of EBV DNA than CD3+ HLA–DR-cells. Real time quantitative PCR for cytokine assessment revealed that interferon-γ, IL-2, IL-10, and TGF-β genes were expressed at higher rate in HLA-DR+ than in HLA-DR T-cells. These results suggested that activated T-cells in chronic active EBV infection expressed high levels of EBV DNA and both Th1 and Th2 cytokines. EBV infected T-cells may contribute to the unbalanced cytokine profiles of infectious mononucleosis. In the present study, out of 17 patients with viral infection, 10 patients showed grade II and 4 had grade III intensity of HP. Only 3 patients had mild HP suggesting that majority of the cases with viral infection had increased severity of HP. Among these patients EBV (08/17), CMV (04/17), Herpes simplex (03/17) and Hepatitis B (02/17) was detected in the screening for virus types.Hemophagocytic syndrome was diagnosed in 7 patients. All of these patients presented with bicytopenia or pancytopenia. Hepatosplenomegaly, liver dysfunction, hyperferritinemia, lipid derangement, coagulation disturbance were concomitant findings of HPS. The bone marrow was mainly hypercellular or normocellular in these cases of HP. The macrophages in the bone marrows of all these patients appeared benign with low nucleus to cytoplasm ratio (N/C ratio), inconspicuous nucleoli in conjunction with abundant cytoplasm. Erythrophagocytosis was mainly present along with phagocytosis of leukocytes and platelets in some of the patients.Hemophagocytosis has been observed in other viral infections as well. Takeoka et al., [23] presented a case of VAHS caused by rubella and Varicella zoster virus as dual infection in patients with idiopathic thrombocytopenic purpura. Liver dysfunction, coagulopathy, hyperferritinemia and thrombocytopenia were reportedly present in their case. Bone marrow examination revealed many atypical lymphocytes and histiocytes with hemophagocytosis [23]. Luppi et al., [24] reported the occurrence of human herpesvirus (HHV)-8 primary infection in an adult male kidney recipient with HP having hemophagocytosis in the bone marrow with peripheral cytopenia [24]. A number of cases have also been reported with hemophagocytosis in relation to hepatitis A. Wantanabe et al., [25] reported hepatitis A with hemophagocytosis in an 18 year old female. The bone marrow smears revealed proliferation of mature histiocytes ingesting platelets and erythrocytes [25]. Most of the patients with viral infection reported so far presented with HPS. In the present study, also, the majority of the patients with viral infection fulfilled the criteria of HPS. Apart from other clinical and biochemical derangements, peripheral cytopenia with increased intensity of HP was an important finding in these patients.Nine patients with tuberculosis were diagnosed in the present study. Six patients had pulmonary and three patients had miliary tuberculosis. Two patients with disseminated TB had granuloma in the BM trephine biopsy specimens. AFB culture in the BM was positive in 2 patients. Three patients presented as hemophagocytic syndrome. Campo et al., [26] reported three patients of HPS associated with tuberculous sepsis. Benign histiocytic proliferation with striking hemophagocytosis was present in all three patients. Fujiki et al., [27] reported a case of HP in a 70 year old female caused by miliary tuberculosis. Laboratory examination revealed anemia thrombocytopenia and liver dysfunction. Bone marrow aspirate revealed tuberculous granulomas and tubercle bacilli by acid fast stains. Histiocytic hyperplasia and hemophagocytosis was also present. 1L-18, sICAM, sVCAM-1 were elevated. They concluded that 1L-18, and adhesions molecules mentioned above play important roles in the pathogenesis of tuberculosis associated hemophagocytic syndrome and correlate with the disease activity [27]. In the present study, patients with tuberculosis with increased intensity, grade III (3cases) had depression of cell counts, including a case of miliary tuberculosis. The authors of present study believe that 1L-18 as seen in previous studies plays an important role to induce peripheral cytopenia particularly by causing secretion of cytokines such as INFγ and TNFα.Thirteen patients with enteric fever were diagnosed in the present study, with variable degrees of HP. Three patients presented as HPS with peripheral pancytopenia, organomegaly and liver dysfunction. One patient had coagulopathy. Erythropoiesis and granulopoiesis were depressed in these patients with histiocytic proliferation and prominent hemophagocytosis in the bone marrow. Blood culture was positive in 5 patients and bone marrow culture for salmonella typhi in 4 patients of enteric fever. Association of erythrophagocytosis with enteric fever is well known and finds support from Risdall et al., [4] who reported three patients with enteric fever having HPS.Nine patients with visceral leishmaniasis were also present in the present study, mostly showing either grade II (5 cases) or grade III (3 patients) HP. One patient presented as HPS. Patient having HPS had severe peripheral cytopenia. Erythropoiesis and myelopoiesis were depressed in this patient. Although an uncommon occurrence, association of visceral leishmaniasis with HPS is well known.In the present study eight (3.2%) patients were diagnosed with malaria. Three patients showed grade II and five patients had grade III HP. Four patients had P. vivax malaria, two had falciparum infection and two patients had mixed infections. Two patients with falciparum infection with grade III intensity presented as HPS with peripheral cytopenia, hepatosplenomegaly, liver dysfunction and hyperferritinimia. Bone marrow in both the patients was hypercellular with depression in erythroid series. Presence of HP in malaria has been scarcely reported in the literature, perhaps because of its uncommon occurrence in the west. Zvulunov et al., [16] reported a case of falciparum malaria with hemophagocytosis resulting in pancytopenia. They proposed that systemic parasitic infections, particularly falciparum malaria, should be included in the differential diagnosis of pancytopenia and infection associated HPS. In the present study also, 2 patients of falciparum malaria had HPS and pancytopenia.The present study includes three adult patients with brucellosis, one having mild and two with moderate HP. Serology was positive for Burcella melitensis and abortis in these patients. None of the patient presented as HPS. However, peripheral pancytopenia was found in one patient. Karakukcu et al., [14] reported 54 children with brucellosis, eight of these patients had pancytopenia with HP. They suggested that hemophagocytosis associated with non viral infection could be related to over production of cytokines such as TNF-α and INF-γ. Bone marrow failure, hypersplenism, granulomas and hypercytokinemia may result in peripheral cytopenia in such patients. It is presumed that pathogenesis of peripheral cytoplasms in infection associated HPS is multifactorial and largely depends upon the type of underlying infection. In viral illness, for example, the antigens may directly target the cells. Other possible mechanisms include hypersplenism, immune destruction of cells, bone marrow infiltration and suppression by microbes, phagocytosis of hemopoietic cells and above all hypercytokinemia. Additional studies are, however, necessary to clarify the possible role of bone marrow microenvironment the pathogenesis of HPS leading to pancytopenia and to investigate in detail the role of T lymphocytes and their associated cytokines profile (Th1/Th2 immune response).
5. Conclusions
- Viral, bacterial and parasitic infections play an important role in the causation of histiocytic hyperplasia with HP. It may present as HPS with multisystem disorder which could be fatal if improperly diagnosed and/or treated. Severe intensity of HP has a profound effect on hematological parameters of patients particularly on hemoglobin levels and platelet count.Early recognition of infection associated HPS is important in deciding supportive measures, treatment of underlying infection and anti-cytokine therapy that may help in saving the patient’s life.
Abbreviations
- Hemophagocytosis = HP; Hemophagocytic syndrome = HPS; X-linked lymphoproliferative syndrome = XLP; Chédiak–Higashi syndrome = CHS; virus associated hemophagocytic syndrome = VAHS; Epstein-Barr virus = EBV; cytomegalovirus = CMV; TGF-β gene = Transforming growth factor beta; Acid- Fast Bacilli culture = AFB culture; total leukocyte count = TLC; TNFα = Tumor necrosis factor; 1L = Interleukin; INF-γ = Interferon –γ; HPF = high power field; soluble intercellular adhesion molecule 1 = sICAM-1; Soluble vascular cell adhesion molecule-1 = sVCAM-1