-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2014; 4(1): 8-13
doi:10.5923/j.ajmms.20140401.02
Seroprevalence and Role of C- Reactive Protein (CRP) Estimation in Chikungunya Positive Cases in Mumbai
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLV. N. Solanke, M. B. Mody, M. G. Karmarkar, P. R. Mehta
Department of Microbiology, Seth G.SMC and KEM Hospital, Parel, Mumbai, 400012, India
Correspondence to: V. N. Solanke, Department of Microbiology, Seth G.SMC and KEM Hospital, Parel, Mumbai, 400012, India.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Introduction:Given the expanding geographic range of chikungunya virus and its potential to rapidly cause large scale epidemics, it has become important to understand the immune and pathogenic mechanisms active during this infection. Levels of C- Reactive Protein (CRP) increase very rapidly in response to trauma, inflammation, and infection and decrease just as rapidly with the resolution of the condition. Thus, the measurement of CRP is widely used to monitor various inflammatory states. Hence, this study was done to know the seroprevalence of chikungunya and to assess the prognostic role of quantitative estimation of C-reactive protein (CRP) in chikungunya positive cases.Materials and Methods:Patients with fever and arthralgia were tested for Chikungunya by IgM antibody capture ELISA. All relevant clinical details were noted. These chikungunya positive samples were then subjected for the quantitative estimation of CRP. On follow up after three months, patients symptoms were noted, CRP estimation was repeated and the difference between these CRP readings was recorded.Results:Out of 630 samples tested, 55 (8.7%) were positive for chikungunya. 23/55 (41.8%) were males and 32/55 (58.1%) were females with 21-40 years age group had maximum patients. The clinical features were fever, joint pain, headache, bodyache, abdominal pain, retro-orbital pain and rash. The average duration of fever was 4 days. The mean CRP level of chikungunya positive cases and follow up cases was 43.13 mg/L and 15.34 mg/L respectively. Of 50 follow up cases, 27 (54%) continued to have a residual joint pain, while 23 (46%) were recovered completely.Conclusion:The chikungunya prevalence in the present study was 8.7%. The age group of 21-40 years was commonly affected, with female preponderance. The common symptoms observed were fever, joint pain, headache and bodyache with average duration of fever of 4 days. Response of raised CRP in acute cases of chikungunya and subsequent fall on follow up suggests the prognostic role of CRP in recovery of patient.
Keywords: Chikungunya, ELISA, C - Reactive Protein (CRP)
Cite this paper: V. N. Solanke, M. B. Mody, M. G. Karmarkar, P. R. Mehta, Seroprevalence and Role of C- Reactive Protein (CRP) Estimation in Chikungunya Positive Cases in Mumbai, American Journal of Medicine and Medical Sciences, Vol. 4 No. 1, 2014, pp. 8-13. doi: 10.5923/j.ajmms.20140401.02.
Article Outline
1. Introduction
- In the recent years, emerging and re-emerging tropical infectious diseases have been shown to cause high social and economic impact. Vector-borne infectious diseases such as Dengue, West Nile fever have been resurging largely due to the spread of insecticide resistance, to socio-demographic changes, and to genetic mutations in the pathogens. More recently, chikungunya fever (CHIKF) has emerged as the next important infection in South-East Asia, the Pacific region and Europe,[1] making it a major threat that requires immediate attention. Since February 2006, an epidemic of chikungunya has affected 8 states in India, with an estimated number of 1.25 million cases[2]. Chikungunya virus (CHIKV) is a positive strand RNA enveloped alphavirus belonging to the Togaviridae family. CHIKV is transmitted by Aedes mosquitoes mainly A. aegypti and A. albopictus and was first isolated by R.W. Ross in the Newala district of Tanzania[3]. CHIKF is an acute illness with abrupt fever, arthralgia, skin rash, and occasional involvement of the nervous system, heart and liver. Prolonged incapacitating arthralgia has sometimes been reported to persist for years. At present, there is no specific or effective treatment for CHIKF, and patient management is largely symptomatic relief primarily with anti-inflammatory drugs[4]. Given the expanding geographic range of CHIKV and its potential to rapidly cause large scale epidemics, it has become important to understand the immune and pathogenic mechanisms active during CHIKV infections. Cytokines and chemokines are thought to play an important role in viral immunopathology of chikungunya. CHIKV induces cellular damage which may lead to secretion of these factors; however, limited studies have been conducted[5]. In cases of chikungunya, no significant pathognomic hematological findings are seen. C - reactive protein is increased during the acute phase and may remain elevated for a few weeks. Leucopenia with lymphocyte predominance is the usual observation. Thrombocytopenia is rare. Erythrocyte sedimentation rate is usually elevated[6]. C-reactive protein (CRP) is an ancient highly conserved molecule and a member of the pentraxin family of proteins. CRP is secreted by the liver in response to a variety of inflammatory cytokines. It binds to damaged tissue, to nuclear antigens and to certain pathogenic organisms in a calcium-dependent manner. Levels of CRP increase very rapidly in response to trauma, inflammation, and infection and decrease just as rapidly with the resolution of the condition. Thus, the measurement of CRP is widely used to monitor various inflammatory states[7].Hence, this study was done to know the seroprevalence of chikungunya and to assess the prognostic role of quantitative estimation of C-reactive protein (CRP) in chikungunya positive cases.
2. Material and Methods
2.1. Study Design, Area and Population
- This prospective study was carried out from January 2013 to September 2013 in a teaching tertiary care hospital in Mumbai. 630 samples from patients of all age group, presenting with fever and arthralgia were included in the study.
2.2. Data Collection
- The relevant clinical information of age, gender, and symptoms was recorded from the requisition form.
2.3. Sample Collection and Processing
- Patient’s blood was collected in plain vacutainer (3 cc) following universal safety precautions. Serum was separated and tested for the presence of IgM antibody for chikungunya using Chikungunya IgM antibody capture (MAC) ELISA. Test procedure and Interpretations were made as per the kit literature. These kits were supplied by National Institute of Virology (NIV), Pune.The samples positive for chikungunya were then subjected for the quantitative estimation of C-reactive protein (CRP) by latex turbidimetry method by using CRP Turbilatex kit (Mfg by Vital Diagnostics, Thane). The CRP level of each chikungunya positive sample was recorded.Follow up of these chikungunya positive patients was done after three months. Patients symptoms were recorded on follow up. Blood samples were collected and subjected for CRP estimation by the same method and CRP levels were recorded.
2.4. Principle and Procedure of ELISA Test
- Briefly, Wells were washed thrice with wash buffer, 50 µl of diluted (1:100 in serum diluent) patient serum, undiluted positive control and negative control, was added to microwells precoated with anti-human IgM antibody and then incubated for 1 h at 37ºC and washed for five times. Then 50 µl of chikungunya antigen was added and incubated for an additional 1 h at 37ºC and then wells were washed five times. Again 50 µl of Anti chikungunya monoclonal antibody was added and incubated for 1 h at 37ºC and washed five times. Avidin HRP 50 µl was added and incubated for 30 min at 37ºC, this was followed by washing the plate five times. TMB/H2O2 (substrate) 100 µl was added and incubated for 10 min at room temperature in dark. The reaction was stopped by adding 100 µl stop solution (1 N H2SO4), and the plates were read at 450 nm.
2.4.1. Calculation and Interpretation of ELISA Results
- If OD value of sample tested was less than OD of Negative control by a factor 2, the sample was considered as ‘Negative’. If OD value of sample tested exceeded OD of Negative control by a factor 3, the sample was considered as ‘Positive’. If OD value of sample tested exceeded OD of Negative control by a factor 2, but was less than OD of Negative control by a factor 3, the sample was considered as ‘Equivocal’. The sensitivity and specificity of MAC ELISA kit is 95% and 98% respectively as mentioned in the literature.
2.5. Procedure of CRP Turbilatex (Quantitative estimation of CRP in serum) Method
- Working reagent was prepared by mixing 9ml of buffer solution and 1ml of latex reagent. Reconstituted calibrator was prepared by adding 1ml of distilled water in CRP calibrator.In 1000µl of working reagent, 5µl of reconstituted calibrator was added and reading was taken in turbidimetry analyzer machine and stored as calibrator reading. Similarly, in 1000µl of working reagent, 5µl of serum was added and reading was taken in turbidimetry analyzer. The calculations were done with the inbuilt formula stored in the analyzer and the level of CRP was obtained in mg/L.
2.6. Ethical Considerations
- The study was approved by the Institutional Ethics Committee (IEC-II) (EC/OA-10/2012). Written informed consent was obtained from all subjects enrolled in the study. Where the participants were minors, written informed consent was obtained from parents or guardian on behalf of all child participants.
2.7. Statistical Analysis
- The data generated from this study were presented using descriptive statistics. The data was subjected to Chi square test for comparison of proportions to determine any significant relationship between chikungunya infection with age and gender. Confidence Interval level was set at p= 0.05. There was a statistically significant difference (p < 0.05) in chikungunya seropositivity between the age and gender.
3. Results
- In this study, out of 630 samples received from clinically suspected chikungunya cases, 55(8.7%) were positive for chikungunya IgM antibody. Of Chikungunya positive patients (55 cases), 23 (41.8%) were males and 32 (58.1%) were females. The most commonly affected age group was 21-40 years (Figure 1). The clinical features were fever and joint pain, followed by headache, bodyache, abdominal pain, retro-orbital pain and rash (Figure 2). The average duration of fever was 4 days. The mean CRP level of chikungunya positive cases was 43.13 mg/L. Out of 55 only 50 patients turned up for the follow up after three months. The symptoms of these patients were recorded on follow up. The mean CRP level of chikungunya positive follow up cases was 15.34 mg/L. It was noted that out of 50 cases, 27 (54%) continued to have a residual joint pain with resolution of all other symptoms (CRP >10mg/L), while 23 (46%) were recovered completely (CRP < 10mg/L) (Figure 3).
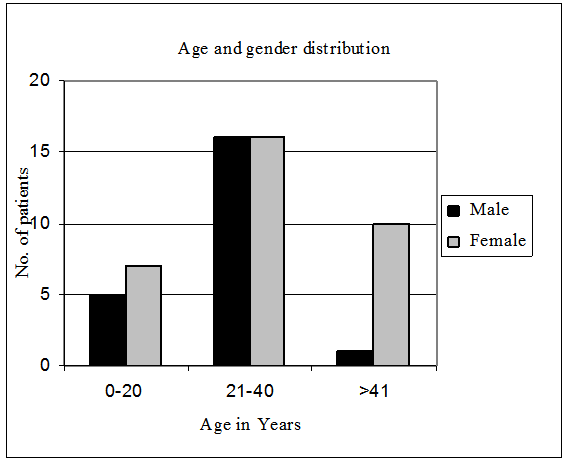 | Figure 1. Age and Gender distribution in Chikungunya |
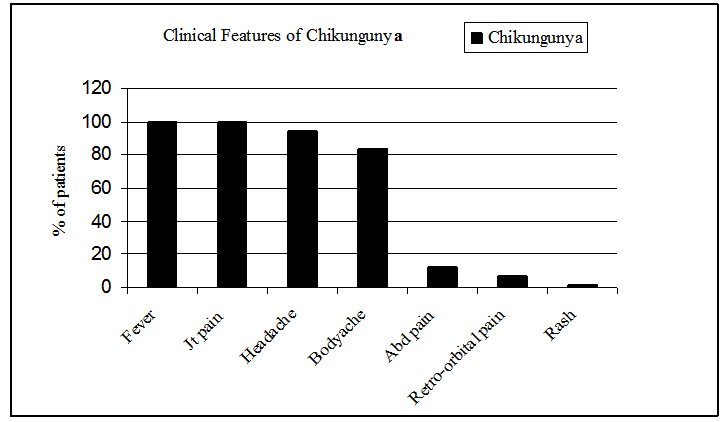 | Figure 2. Clinical Features of the patients with Chikungunya |
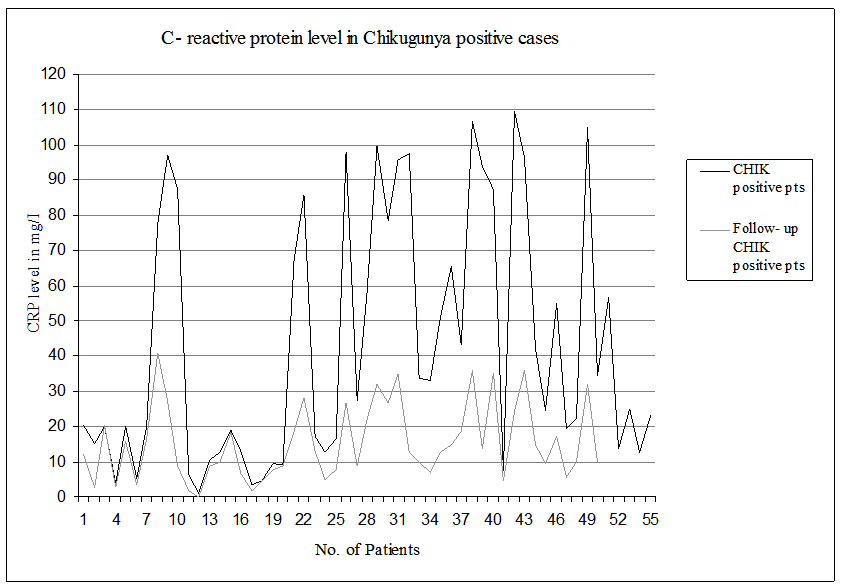 | Figure 3. C-reactive protein levels in Chikungunya positive cases |
4. Discussion
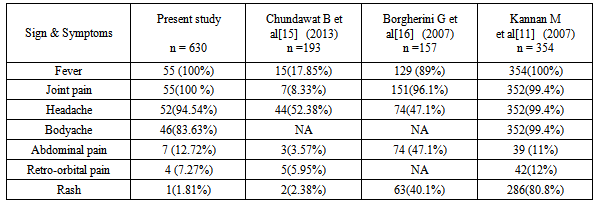
- In recent years, countries in the South-East Asia Region have been severely affected by the outbreaks of chikungunya fever. India was hit in 2006 after quiescence of 32 years. Indonesia, Maldives, Sri Lanka and Thailand have also been swept by this emerging infection. Various factors that have been incriminated to resurgence of chikungunya include mutation of the virus, absence of herd immunity, lack of efficient vector control activities, globalization and emergence of Aedes albopictus, in addition to Aedes aegyptii as an efficient vector for chikungunya virus. Proposed case definition of Chikungunya Fever (WHO, SEARO)[8]. Criteria for diagnosis: 1. Clinical criteria: acute onset of fever >38.5°C and severe arthralgia/arthritis not explained by other medical conditions 2. Epidemiological criteria: residing or having visited epidemic areas, having reported transmission within 15 days prior to the onset of symptoms 3. Laboratory criteria: at least one of the following tests in the acute phase: - Virus isolation - Presence of viral RNA by RT-PCR - Presence of virus specific IgM antibodies in single serum sample collected in acute or convalescent stage. - Four-fold rising of IgG titers in samples collected at least three weeks apart.Case definition for surveillance: Possible case: a patient meeting clinical criteria Probable case: a patient meeting both the clinical and epidemiological criteriaConfirmed case: a patient meeting the laboratory criteria, irrespective of the clinical presentationIn the present study, when a single sample was collected in acute stage of the disease and tested for the presence of chikungunya virus specific IgM antibodies by MAC ELISA, 8.7% samples were positive for chikungunya.In our study, the commonest age group affected was 21-40 years with maximum 32 patients belonged to this group (Chi square value= 8.472 with DF-1, p value=0.0036, statistically significant). Same findings were also seen in studies by Lakshmi V et al.,[9] Suryawanshi SD et al.,[10] and Kannan M et al.,[11] where the common age group affected was 31-40 years, 21-30 years and 16-35 years respectively. However, the study conducted by Sharma et al during the outbreak in Madras city in 1964 showed that the population belonging to the age group 5-9 years had the highest percentage of morbidity (23.2%)[12]. We have seen that in chikungunya male: female (M:F) ratio was 1:1.6. Females were more commonly affected (Chi square value=5.720 with DF-1, p value=0.0168, statistically significant) and this female preponderance may be due to the fact that females continued to be present in their houses more than males[13]. Similar results were comparable with Chakravarti A et al.,[14] and Chundawat B et al.,[15] where M:F ratio was 1:1.34 and 1:1.62. However, in the study conducted by Sharma et al.,[12] and Borgherini G et al.,[16] it has been reported that the males were more frequently affected than females. The average duration of fever was 4 days which is similar to the report by Sharma et al.,[12] and Thiruvengadam et al.,[17] Fever and joint pain was the most common symptom (100%) followed by headache, bodyache, abdominal pain, retro-orbital pain and rash (Table 1).
|
5. Conclusions
- The chikungunya prevalence in the present study was 8.7%. The age group of 21-40 years was commonly affected, with female preponderance. The common symptoms observed were fever, joint pain, headache and bodyache with average duration of fever of 4 days. Response of raised CRP in acute cases of chikungunya and subsequent fall on follow up suggests the prognostic role of CRP in recovery of patient.
ACKNOWLEDGEMENTS
- We thank Research Society of our Institute for Financial support. We also thank Joint Director Health Services, Pune and National Institute of Virology (NIV), Pune for providing chikungunya ELISA kits through National vector borne disease control programme (NVBDCP).