-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2012; 2(3): 59-61
doi: 10.5923/j.ajmms.20120203.06
Dextrocardia With Situs Inversus Totalis in an Adult Nigerian: a Case Report
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-Text HTML
Full-Text HTMLUchenna DI , Jesuorobo DE, Anyalechi JI
Department of Internal Medicine, University of Port-Harcourt Teaching Hospital, Port-Harcourt. Nigeria
Correspondence to: Uchenna DI , Department of Internal Medicine, University of Port-Harcourt Teaching Hospital, Port-Harcourt. Nigeria.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Situs inversus with dextrocardia is the complete inversion of position of the thoracic and abdominal viscera. It may be isolated or associated with malformations, especially cardiac or alimentary. It may be discovered in infancy because of associated anomalies but often remains asymptomatic and discovered by chance in adult life. We report a 69 year old Nigerian woman found to have dextrocardia with situs inversus totalis while presenting for treatment for a totally unrelated problem. Her chest radiograph was however erroneously marked by the radiographer as normal resulting in a wrong report. The findings from an electrocardiogram and echocardiography confirmed the location of the heart in the right hemithorax and an abdominal sonogram showed the liver and gall bladder on the left side of the abdomen while the stomach and spleen were located on the right side. This report underscores the need for routine screening by individuals so that such congenital anomalies can be identified and surgical diagnoses in such patients made correctly to prevent surgical complications.
Keywords: Dextrocardia, situs inversus, Malformation, electrocardiogram, Nigerian
1. Background
- Dextrocardia is an abnormal congenital positioning of the heart. Instead of the heart forming in the fetus on the left side, it flips over and forms on the right side1 Situs inversus (also called situs transversus) is a congenital condition in which the major visceral organs are reversed or mirrored from their normal positions. Many people with situs inversus totalis are unaware of their unusual anatomy until they seek medical attention for an unrelated condition Dextrocardia is frequently diagnosed in a routine prenatal sonogram, although not every radiologist will identify it, particularly if there are no cardiac structural abnormalities2 Diagnostic modalities like a chest radiograph and an electrocardiogram are sufficient to make a diagnosis of dextrocardia while more recent imaging modalities like echocardiography and magnetic resonance imaging puts the diagnosis beyond doubt. We report a peculiar case of dextrocardia with situs inversus in a 69 year old woman whose chest radiograph was erroneously labelled by the radiographer as normal.
2. Case Report
- Mrs C.I. is a 69 year old woman who presented to the general outpatient clinic of the University of Port Harcourt Teaching Hospital with complaints of back pains as well as pains in both knees which has been recurrent for the past year. There was no history of cough or chest pains but admitted to occasional exertional dyspnea. She is neither hypertensive nor diabetic and does not smoke cigarettes. She was sent for some tests including a chest radiograph and an electrocardiogram (ECG). The chest radiograph was reported as normal though an alteration was noticed on the film where the left maker was cancelled from its initial position and transferred to the opposite side of the film (Figure 1). The left sided ECG however demonstrated negative P wave deflection in leads I and aVL with R wave regression in the precordial leads – mirror image of normal. Though the P waves were inverted in leads I and aVL of the right sided ECG, R wave progression in the precordial leads was normal (Figure 2). The right sided ECG also showed left ventricular hypertrophy using the Sokolow-Lyon criteria (Figure 3).
 | Figure 1. Chest radiograph of a 69 year old lady with dextrocardia and situs inversus showing the cardiac apex in the right hemithorax with the gastric bubble visible in the right upper quadrant |
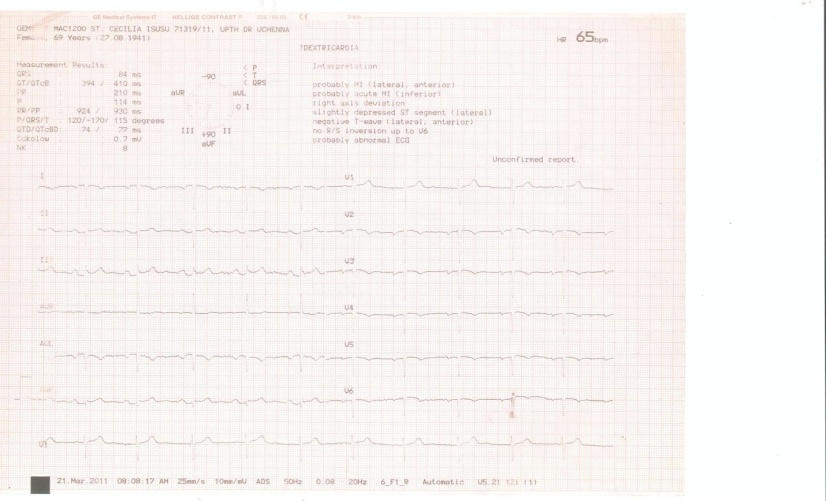 | Figure 2. Electrocardiogram of our patient with dextrocardia showing sinus rhythm with right axis deviation, inverted P waves in leads I, aVL and aVR as well as predominantly downward QRS complexes in leads I, V5 andV6. |
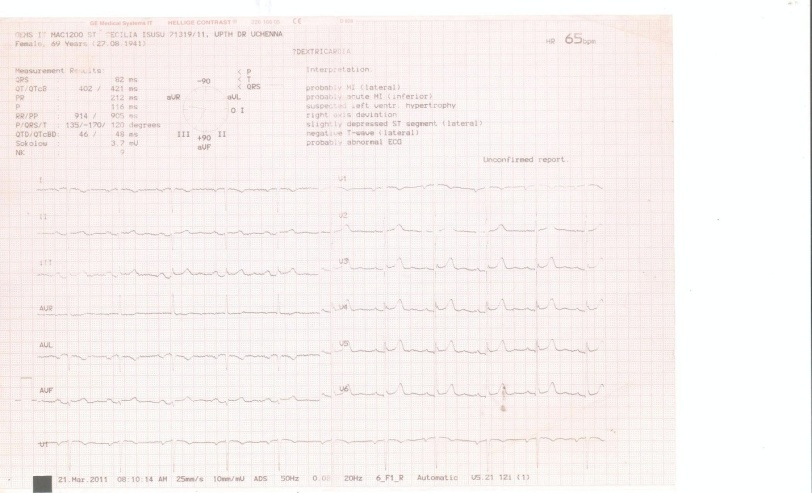 | Figure 3. Electrocardiogram of the same patient with the chest leads reversed still showing inverted P-waves in leads I, aVL and aVR but a normal R wave progression on the chest leads |
3. Discussion
- Dextrocardia with situs inversus is a rare condition occurring in about one per 10,000 in the general population There is no racial predilection for situs inversus and the male-to-female incidence is 1:1. This anomaly may not be diagnosed until late in life in some cases and it is associated with primary ciliary dyskinesia and splenic malformations in some individuals3 The arrangements of the position of the abdominal viscera in dextrocardia may be normal (situs solitus), reversed (situs inversus), and indeterminate (situs ambiguous or isomerism) in 32-35%, 35-39% and 26-28% of cases respectively4 Though the exact cause is unknown, dextrocardia has been linked with a number of factors including autosomal recessive gene with incomplete penetrance, maternal diabetes, cocaine use and conjoined twinning.5,6 The mechanism responsible for malrotation of intestinal loops is yet to be understood. Evidence from the literature had it that the direction of rotation is under influence of forces exerted by adjacent organs on intestines and its mesentery7Dextrocardia with a normal abdominal situs has a high incidence of associated congenital cardiac anomalies including among others, transposition of the great vessels and atrial8 and ventricular septal defects9 in 90-95% of cases. On the other hand, dextrocardia with situs inversus is associated with a lower incidence of congenital heart disease (0-10%) and as such, relatively asymptomatic, as was the case in our patient. In the rare instance of cardiac malformations, life expectancy is reduced depending on the severity of the defect. Non cardiac malformations, on the other hand, occur in the same population in situs inversus and ambiguous. One such non-cardiac malformation is the combination of dextrocardia, abnormality of mucociliary function and bronchiectasis (Kartagener’s syndrome) which has been reported in a Nigerian child and is associated with repeated sinus and pulmonary infections.Several cases of dextrocardia have been documented in Nigeria, some with co-existing cardiac anomaly while others were asymptomatic or had non cardiac symptomatic malformations10-14 The recognition of situs inversus is important for preventing surgical mishaps that result from the failure to recognize reversed anatomy or an atypical history. For example, in a patient with situs inversus, cholecystitis typically causes left upper quadrant pain15 Situs inversus also complicates organ transplantation operation as donor organs will almost certainly come from situs solitus (normal), as heart and liver have geometric problems while placing the organs into a cavity shaped in mirror image. The orientation of these blood vessels are also reversed, necessitating steps to be taken so that blood vessels join properly Diagnosis of dextrocardia with situs inversus can be confirmed by several modalities including chest radiography, electrocardiography, echocardiography, computerized axial tomography scans, magnetic resonance imaging and abdominal ultrasonography.
4. Conclusions
- Dextrocardia with situs inversus is a rare congenital malformation that must be fully evaluated when noticed as it is in most instances associated with normal life expectancy as in the case of the index patient. There is need for a complete and elaborate diagnostic work up of suspected cases by various imaging modalities so that they are not missed. The electrocardiogram gave away the diagnosis in our patient which led us to question the accuracy of the report of the chest radiograph. Surgeons, radiologists and radiographers should look out for this anomaly during preoperative and surgical management of their patients. Doctors should encourage routine medical examination for their patients which could help identify this anomaly, thereby preventing wrong diagnosis and possibly death due to delay in management.