-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Dermatology and Venereology
p-ISSN: 2332-8479 e-ISSN: 2332-8487
2025; 14(1): 1-5
doi:10.5923/j.ajdv.20251401.01
Received: Jan. 6, 2025; Accepted: Feb. 2, 2025; Published: Feb. 6, 2025

Quality of Life among Sudanese Patients with Vitiligo
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSarah Fuad Thabit1, Basel Adel Basrawi1, Alamin Mustafa Eltayeb1, Amira Ibrahim Hassan1, Mahdi Shamad2
1Student at Faculty of Medicine, Al-Neelain University, Sudan
2Associate Professor of Dermatology and Venereology, College of Medicine, University of Bahri, Sudan
Correspondence to: Mahdi Shamad, Associate Professor of Dermatology and Venereology, College of Medicine, University of Bahri, Sudan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

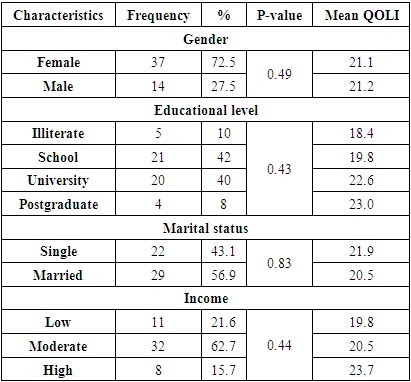
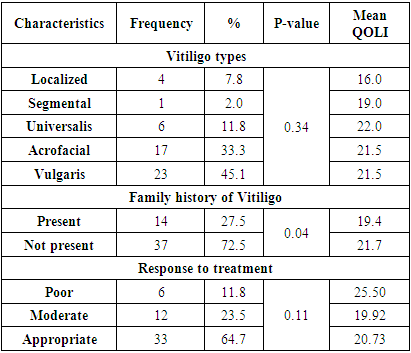
Introduction: Vitiligo is a dermatological disease affecting the melanocytes and causing white skin patches on different body areas that may affects the quality of life (QOL). Rapidly progressed vitiligo despite the treatment may increase the phycological impact of the disease. Methods: This was cross-sectional, hospital based study conducted among 51 vitiligo patients at Al Khalifa Suleiman dermatology hospital. Data was collected via a closed-ended interview using paper-based questionnaire that include different demographics and QOL questions that were extended from dermatological life quality index (DLQI), we added 6 more questions according to study objectives and the score was maximally 48. The data was analysed using SPSS version 26. Descriptive data was shown as median and interquartile range. Kruskal-Wallis Test and Whitney U test was used to assess the impact of Vitiligo types and its progression on Quality of Life Index (QOLI), any p ≤0.05 was considered statistically significant. Result: The mean of the patients ages were 32.3 years. 37(72.5%) of the patients` were females while 14 (27.5%) were males, 22 (43.1) were single while 29 (56.9%) were married. The common types of Vitiligo in the study were vulgaris 23 (45.1%), Acrofacial 17(33.3%) and Universalis 6 (11.8%). Localized 4 (7.8%) and segmental 1 (2.0%) types were less common. The mean duration of having Vitiligo is 11.24 ± 9.7 years and no correlation was found between quality of life index (QOLI) and the duration of having Vitiligo (p-value >0.27). Comparison between QOLI and gender was statistically insignificant (p value >0.05). Both Vitiligo progression and family history of Vitiligo affected the quality of life (P value <0.05). QOLI was not affected by the Vitiligo type (P value >0.05). Conclusion: Although the impact of Vitiligo on QOL does not depend on the gender or marital status of the patients, it is affected by the disease progression and family history.
Keywords: Vitiligo, Quality of life, Sudan
Cite this paper: Sarah Fuad Thabit, Basel Adel Basrawi, Alamin Mustafa Eltayeb, Amira Ibrahim Hassan, Mahdi Shamad, Quality of Life among Sudanese Patients with Vitiligo, American Journal of Dermatology and Venereology, Vol. 14 No. 1, 2025, pp. 1-5. doi: 10.5923/j.ajdv.20251401.01.
Article Outline
1. Introduction
- Vitiligo is an acquired skin disorder characterized by loss of melanocytes in the epidermis [1]. It has low prevalence worldwide and can affect any body at any age with various distribution patterns [2]. Psychological problems can increase the incidence and progression of the disease and disrupt the patient’s life [2], the etiology is not clear and there is no definitive treatment when the study was conducted [3,4,5]. Vitiligo affects the quality of life (QOL) in various degrees in different communities. However, In Sudan it is considered as stigma, so it is difficult to live with the disease which affects self-confidence and the ability to marry or having normal life. Studies from Europe [6-8] and Asia [1,9,10] were done. For instance, in Malaysia there was a moderate reducing in QOL of Vitiligo patients [10]. In South Africa they used dermatological life quality index (DLQI) score and the mean was of 10.67 [11]. In Sudan a study was conducted at Khartoum dermatology hospital that found that Vitiligo is responsible for psychological problems in large number of patients [12]. The impact of Vitiligo on quality of life is severe in many affected individuals, and it is critical for physicians to recognize this aspect of the condition and address their patients’ psychological needs. It is clear that the impact of skin diseases on people’s lives is not often appropriately considered in their treatment, and in general the management of their condition usually focuses on clinical signs and symptoms and not on a subjective view of the impact of the disease on the patient life especially the social relationships. In Africa, few studies on QOL and skin diseases in general and on Vitiligo in particular have been undertaken [4]. In Sudan Vitiligo is rare with a consequent impairment of quality of life. However, studies on quality of life impairment, the clinical and socio-demographic factors which affect their quality of life, very few attempts were conducted to investigate the impact of the Vitiligo progression overtime and the QOL among Vitiligo patient`s in Sudan. In addition, no previous studies were conducted to assess and compare between patient`s QOLI with different types of Vitiligo and its progression overtime. This study aim to answer the question of how much the quality of life of Vitiligo patients is affected as the disease progressed and what type of Vitiligo affected the patient QOL most. This study assessed the QOL in Vitiligo patients, considering the impact of disease progression, types and patients gender on the QOL.
2. Patients and Methods
- This was cross-sectional, hospital based study conducted at Al-Khalifa Suleiman dermatology hospital, Omdurman province, Khartoum state, Sudan. The hospital considered as national referral hospital for Vitiligo treatment using phototherapy and photochemotherapy procedure, which were not available in many dermatology clinics nationally. The study was conducted between March to May 2022. The population of this study was all Vitiligo patients who did not suffer from other dermatological disease and attending the hospital during the study period and achieving the study criteria, the minimum sample size needed was calculated using the hospital-based prevalence of Vitiligo in Africa 3.4% [21] and using 95% confidence interval (CI) and 5% precision, those numbers are plotted in Danial`s sample size formula by prevalence, the sample size was 51 patients.
2.1. Data collection Tools and Informed Consent
- Data was collected via a closed-ended interview using paper-based questionnaire that include different demographics and quality of life (QOL) questions that were extended from the dermatological life quality index (DLQI) and we added 6 more questions according to study objectives and the score was maximally 48. (18 scores more than DLQI) this methods enable better statistical conclusions despite small sample size; otherwise everything is similar to DLQI. For Vitiligo progression, the patients were asked about how Vitiligo was progressed on the last six month before interviewing them and how its progression affected their Quality of Life Index (QOLI) was examined using the modified DLQI scale. Different Vitiligo types have been investigated by professional dermatologist doctors and then the Vitiligo types were reported on the patient questionnaire. The authors explained to patients the aim of the study and participating or refusing will not influence their treatment at the hospital. The authors insured that the patients understood the information given and because some patients were illiterate informed consent was obtained verbally before enrolling to the study and informed consent from children who suffer from Vitiligo was obtained from their parents and all patients allowed asking questions at any time. The confidentiality of the participants was established by coding the questionnaires and was considered throughout the study.
2.2. Statistical Analysis
- The data was entered and analysed by SPSS version 26. Descriptive data was shown as median interquartile range and mean ± standard deviation, the general characteristics of the participants was shown in frequency and percentages. The Spearman`s rank correlation test was used for revealing the correlation between categorical and quantitative data. Moreover, Kolmogorov-Smirnov test was used for normality examination and Mann-Whitney U test was used to compare between male and female quality of life (QOI). The nonparametric Kruskal-Wallis Test was used to compare the quality of life index (QOLI) across subgroups variables (Vitiligo progression, types of Vitiligo and patients income). The Correlation between each categorical data was revelled by using chi-square test for independence and any p value ≤ 0.05 was considered to be statistically significant “two-tailed unless otherwise mentioned”.
3. Results
- The demographic data of the study population and the relation with Quality of Life Index (QOLI) is shown in Table 1.
|
|
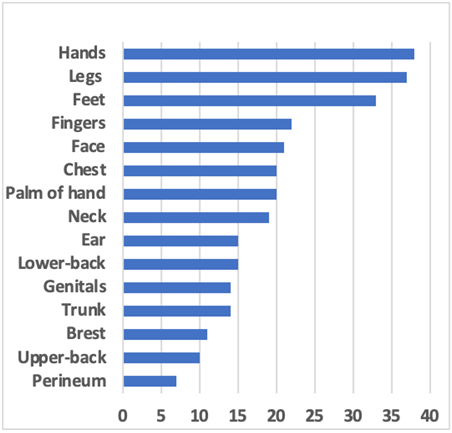 | Figure 1. The frequency of the affected regions of the body by Vitiligo |
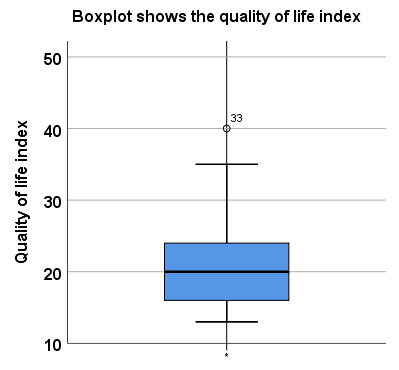 | Figure 2. The distribution of the quality of life index (QOLI) among Vitiligo patients |
 | Figure 3. The quality of life index by vitiligo type and gender |
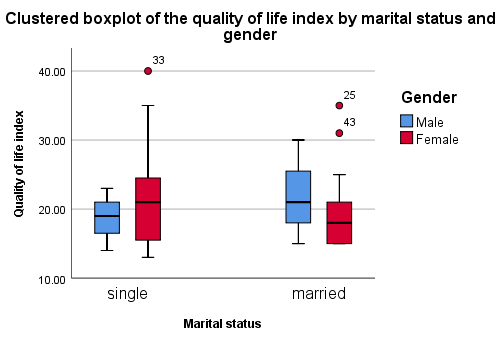 | Figure 4. The quality of life index by patients` marital status and gender |
|
4. Discussion
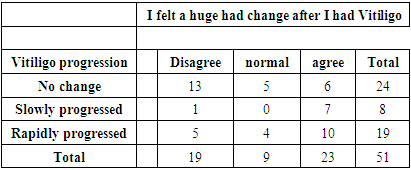
- In this study, we used quality of life index (QOLI) ranged from 0 to 48 with decrease in the quality of life (QOL) by increase in the score. The mean duration of having Vitiligo is 11.24 ±9.7 years; the study found that the Vitiligo has a slightly low effect on the QOL of the patients. The total mean for QOLI in this study = 21.09. For us, gender was the most interesting thing to see its effect on QOL on the Vitiligo patients especially after reading studies said that females are more concerned about the disease, and they are getting medical services more than men [8,13,14]. Females n= 37 (75%) and males n=14 (27.5%). Surprisingly, there was not a significant effect of gender on QOL of Vitiligo patients. This result was compatible to studies done in South Africa and Iran [11,22]. In Germany and Iran, they found that men and women with Vitiligo have different QOLs [15,16]. We also found that there is not a significant relation between gender and marital status, and marital status douse not affect the QOL impairment. In Saudi Arabia and India, married subjects have less QOL impairment compared with single or divorced patients [1,10]. Patients with family history of Vitiligo were n=13 (17%). In Johannesburg were n=18 (18.95%) and in France were about n=11 (23%) [11,19]. Unlike V. Ingordo in Italia and Elisah Agaba in Johannesburg [11,17] it was found that there is significant relation between QOL and family history of Vitiligo [11]. Unlike study made in India, founded that progression of Vitiligo was significantly associated with QOL impairment [10]. For study patients, duration of the disease has no significant relation to QOL. Other studies found that the duration affect the QOL of the patients [8,18]. This study found that there is no significant relation between the treatment modality that taken by the patient (phototherapy, topical steroid) and the QOL improvement. This finding was compatible with Elisa Agaba and contras with Wong et al year [R] studies [11,20]. Due to religion and traditions, Affected areas like Face n=21 (41.17%), Neck n=19 (37.25%) and Hands n=38 (74.50%) are mostly the only exposed body areas in Sudan. Many studies including ours show that there is not a significant relation between exposed areas and QOL. But studies done by wong and Baba in Malaysia found that there is a significant relation between QOL and exposed areas. However most of the patients in our study said that they did not put any cosmetics to hide the exposed patches.
5. Strength and Limitation of This Study
- This study has limitations, it was done at a single centre and the sample size was too small to be representative, therefore may not show the real impact of Vitiligo on the quality of life (QOL) of all Sudanese with the condition. Nevertheless, there are only 3 dermatology centres in Sudan which might decrease the chance of bias. Future studies could include the other centres and employ stratified sampling strategy, as well as increase the sample size, to be more representative. There was not a control condition or comparisons. Hence, future studies should aim to compare clinical data with data collected from healthy populations. This was a cross-sectional study so we could not identify the causality. However, to our knowledge, studies in Sudan looking at the QOL of patients suffering from Vitiligo are very few. Future research should be longitudinal to explain how variables affect QOL over time having Vitiligo. Most of participants in this study didn’t show an expected social avoiding behaviour.
6. Conclusions
- Vitiligo can affect patient’s quality of life because it disturb the cosmetic appearance of the patient. Counselling the patient and its family is important, in addition to psychological and medical therapy.
Ethical Approval and Consent to Participate
- Ethical approval was obtained from Institutional Review Board at Bahri University.
Funding
- No fund was obtained.
Conflict of Interest
- No conflict of interest.
ACKNOWLEDGMENTS
- Authors are grateful to Dr Shamed for his supervision and permission of submission and reviewing the manuscript and publication. Special thanks to Dr Mona who helped us during the process of data collection and management. Thanks to all patients and their families who without them this study would not be exist and thanks for their time during interviewing.
Abbreviations
- DLQI: Dermatological Life Quality IndexQOL: Quality of LifeQOLI: Quality of Life IndexSPSS: Statistical Package for the Social Sciences