-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Dermatology and Venereology
p-ISSN: 2332-8479 e-ISSN: 2332-8487
2020; 9(4): 51-54
doi:10.5923/j.ajdv.20200904.02
Received: May. 10, 2020; Accepted: Jul. 3, 2020; Published: Oct. 15, 2020

Pattern of Skin Diseases among Medical Students: A Study in Cumilla Medical College, Cumilla, Bangladesh
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLHoq AJMS1, Sultana F.2, MJ Abedin1, GM Matiur Rahman1
1Assistant Professor, Dept. of Dermatology and Venereology, Cumilla Medical College Hospital, Cumilla, Bangladesh
2Emergency Medical Officer (EMO), Mymensingh Medical College Hospital, Mymensingh, Bangladesh
Correspondence to: Hoq AJMS, Assistant Professor, Dept. of Dermatology and Venereology, Cumilla Medical College Hospital, Cumilla, Bangladesh.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Introduction: The pattern of skin diseases differs from one country to another and crosswise diverse parts within the same country. The prevalence of skin disease in the over-all population varies from 11.16% to 63%. Patients in their second and third decades of age form the largest group of residents. The aim of the study was to determine the pattern of Skin Disease among medical Students in Cumilla Medical College, Cumilla, Bangladesh. Material & Methods: This was a Retrospective type of study was conducted in the department of Dermatology of Cumilla Medical College, Cumilla Bangladesh during the period from January 2018 to December 2018. A total number of 587 students were selected as a study population. Among them 214 patients were male and 373 patients were female. Results: A total number of 587 patients had selected for the study. Majority of them were female 373(64.55%) and 214(36.45%) were male. According to type of infective disease majority 70(11.92%) were infected into scabies followed by tinea infection 63(10.73%), Pityriasis versicolor 19(3.23%) and pyoderma 25(4.25%). According to type of non-infective disease. Eczema emerged as the commonest group of disorders 80(13.62%) followed by psoriasis 18(3.06%), acne vulgaris 53(9.02%), urticaria 36(6.13%) and miscellaneous 76(12.95%). Conclusion: A huge problem of skin diseases is existing mostly bacterial and parasitic. Among the infectious diseases we found most of the infective cases were with scabies and tinea infection. On the other hand, most of the non-infective cases were found with eczema only.
Keywords: Skin Disease, Dermatology, Scabies, Medical Students
Cite this paper: Hoq AJMS, Sultana F., MJ Abedin, GM Matiur Rahman, Pattern of Skin Diseases among Medical Students: A Study in Cumilla Medical College, Cumilla, Bangladesh, American Journal of Dermatology and Venereology, Vol. 9 No. 4, 2020, pp. 51-54. doi: 10.5923/j.ajdv.20200904.02.
Article Outline
1. Introduction
- Skin diseases are very much prevalent in the developing countries. [1] The pattern of skin diseases varies from one country to another and across different parts within the same country [2]. These diseases range from simple acne and scabies to various serious disorders such as Stevens Johnson syndrome, toxic epidermal necrolysis and purpura fulminans. [3,4] The prevalence of skin disease in the general population varies from 11.16% to 63% as seen in various studies. [2] Patients in their second and third decades of age form the largest group of population (3.7 percent to 51.17 percent). [5] Skin diseases account for a significant public health issue in developing countries affecting 20-30% of the general population at any given time [6]. The development of skin disease is influenced by various factors like genetic, race, religion, socioeconomic status, nutrition, personal habits, age etc. [7] Geographical factors such as season and climate also contribute to the increased prevalence of certain type of skin disorder in a particular area. [8] The pattern of skin diseases differs between countries and even within regions as a result of these factors. [9] Skin diseases can cause high morbidity but apparently less mortality. It is very important to remember that skin manifestations may be a clue as to the patient’s internal disease, but literature on the pattern of skin diseases is deficient. Early identification of skin disease is important not only for treating patients but for preventing the spread of communicable diseases. [1] Improvements to environmental sanitation, education of the general public awareness regarding personal hygiene and healthy living is necessary to reduce the burden of skin diseases and for improved quality of life in people especially in developing nations. Prescription writing is a science and art, as its conveys the message from the prescriber to the patient. [10] Improvements to environmental sanitation, education of the general public and good nutrition can help to reduce the incidence of skin disorders in any community, [11,12,13] Although there have been some studies on the pattern of skin diseases in the general global population, there is a paucity of such work in developing countries. [11,13,14]
2. Objectives
- To determine the pattern of Skin Disease among Medical Students in Cumilla Medical College, Comilla, Bangladesh.
3. Methodology and Materials
- This was a Retrospective type of study was conducted at the department of Dermatology of Cumilla Medical College of Bangladesh during the period from January 2018 to December 2018. A total number of 587 students were selected as a study population. Among them 214 patients were male and 373 patients were female. Cases with doubtful diagnosis were excluded from the study. Diagnosis was made on clinical basis. Lab investigations were done whenever required to the cases where it carried diagnostic importance. Data were collected from medical record book.. Data analysis performed by SPSS.
4. Results
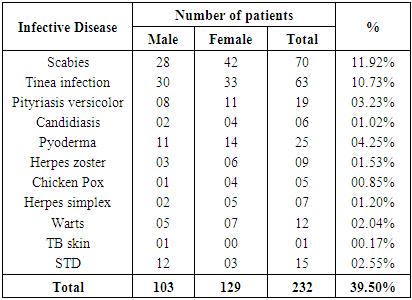
- A total number of 587 patients had selected for the study. (Table 1) shows the gender distribution of our patients’ majority of them were female 373(64.55%) and 214(36.45%) were male. (Table 2) shows the distribution of patients according to type of infective disease. Majority 70(11.92%) were infected into scabies followed by tinea infection 63(10.73%), Pityriasis versicolor 19(3.23%) and pyoderma 25(4.25%). (Table 3) shows the distribution of patients according to type of non-infective disease. Eczema emerged as the commonest group of disorders 80(13.62%) followed by psoriasis 18(3.06%), acne vulgaris 53(9.02%), urticaria 36(6.13%) and miscellaneous 76(12.95%).
|
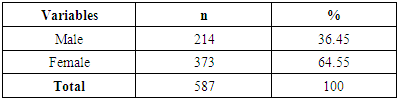
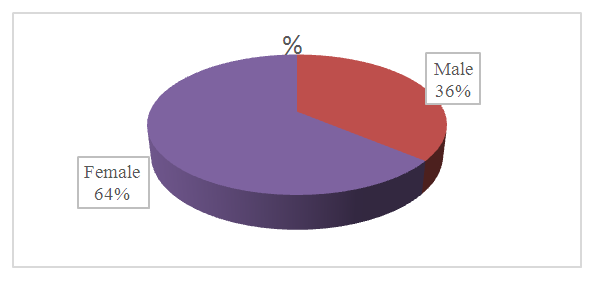 | Figure 1. Distribution of patients according to gender (n=587) |
|
|
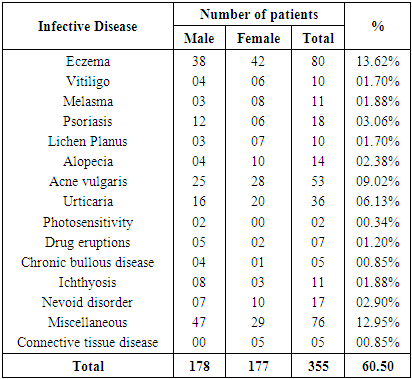
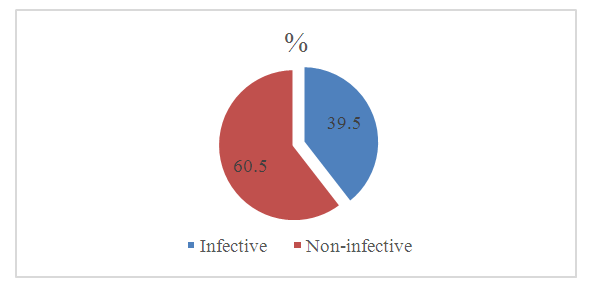 | Figure 2. Distribution of the patients according to type of infective & non-infective disease (n=587) |
5. Discussion
- In this study we found, infective diseases (39.50%) were more than non-infective diseases (60.50%). In Indian sub-continent infectious skin diseases are more common than non-infectious diseases [15-17]. Although in Denmark, Egypt and in Singapore dermatoses are more common and in UK pre malignant and malignant skin diseases are more common [17-20]. Female patients were found more in infectious cases 55.60%, and male patients were found in non-infectious cases 50.14%. In infectious disease parasitic diseases were more common. This is similar to Indian study [13,22-24] but differ from Singapore and Egyptian study [20,19]. Regarding parasitic diseases scabies and pediculosis were most common. But in few Indian study they only mentioned about scabies was more prevalent [13,21-23]. In this study, infective disease majority 70(11.92%) were infected into scabies followed by tinea infection 63(10.73%), Pityriasis versicolor 19(3.23%) and pyoderma 25(4.25%) was found more common. This is similar to one Indian study [23]. In our study, non-infective disease eczema emerged as the commonest group of disorders 80(13.62%) followed by psoriasis 18(3.06%), acne vulgaris 53(9.02%), urticaria 36(6.13%) and miscellaneous 76(12.95%). However, most of the result from the Indian subcontinent shows similar to the present study result. In a study Jain et al 9 have reported that fungal infections is the most common skin disease which is in 54.52% and eczemas is in 39.2%. Again, in another study by Rao et al 1 showed fungal diseases to be the most common infection (22.92%) and eczemas took an upper hand in noninfectious group (32.19%). Likewise, Jain et al 9 have reported that maximum patients presented with eczema of which the most common noninfectious dermatoses (22.0%) and fungal infections are the most common infective dermatoses (13%). However, in developed countries the scenario was different [17-20]. By review various reports, we find that almost all studies mentioned here [25-28] are compatible with our reports i.e., the commonest skin disease is of infective origin, followed by allergic diseases except two reports, [29,30] which show the reverse situation. For infective dermatoses, by reviewing different studies, [25,30,31] it is clear that the fungal or bacterial infections are the commonest infective skin disorder, instead of parasitic and protozoal infestations of our study.
6. Limitations of the Study
- It was a retrospective type of study with small sample size, which doesn’t reflect the scenario of the whole country.
7. Conclusions and Recommendations
- A huge problem of skin diseases is existing mostly bacterial and parasitic. Among the infectious diseases we found most of the infective cases were with scabies and tinea infection. On the other hand, most of the non-infective cases were found with eczema only. Based on the outcome of this study, the common skin problems existing in this area are to be carefully looked for and health education regarding the hygiene, nutrition and healthy life styles is to be stressed for better standard of living.