-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Dermatology and Venereology
p-ISSN: 2332-8479 e-ISSN: 2332-8487
2020; 9(3): 38-42
doi:10.5923/j.ajdv.20200903.02
Received: July 5, 2020; Accepted: August 7, 2020; Published: August 29, 2020

Topical Sesame Seed and Pumpkin Seed Oils have Therapeutic and Prophylactic Role in the Management of Recurrent Aphthous Stomatitis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKhalifa E. Sharquie1, Adil A. Noaimi1, Douaa S. Ahmed2
1Department of Dermatology, College of Medicine, University of Baghdad, Iraqi and Arab Board for Dermatology and Venereology, Baghdad Teaching Hospital, Medical City, Baghdad, Iraq
2Center of Dermatology, Baghdad Teaching Hospital, Medical City, Baghdad, Iraq
Correspondence to: Khalifa E. Sharquie, Department of Dermatology, College of Medicine, University of Baghdad, Iraqi and Arab Board for Dermatology and Venereology, Baghdad Teaching Hospital, Medical City, Baghdad, Iraq.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Recurrent aphthous stomatitis (RAS) is a major oral health problem, where its etiopathogenesis is not well understood. Accordingly, its therapy whether topical or systemic can induce clearance, but the relapse rate is high. Objective: To evaluate the efficacy and prophylactic effects of topical Sesame seed oil in comparison with Pumpkin seed oil in the management of recurrent aphthous stomatitis. Patients and Methods: This is a single, blinded, clinical, therapeutic, comparative study where 45 patients with early onset RAS were recruited in Center of Dermatology -Baghdad Teaching Hospital, Baghdad, Iraq from April 2018-October 2019. Full history and clinical examination were done for each patient and patients were divided into 2 groups: Group A (20 patients) used crude Sesame seed oil twice daily. Group B (25 patients) was instructed to use Pumpkin seed oil in a similar way to Group A. Short term assessment of each patient of both groups was done to evaluate the therapeutic effect of drug by using oral clinical manifestation index (OCMI). A long term assessment was done for each patient to evaluate the prophylactic effect of drug by using OCMI before, after 1, 2 and 3 months of therapy. Results: The patients enrolled in this study were 30 males (66.6%) and 15 females (33.3%), with male to female ratio were 2:1. Their ages ranged between 9-60 (36.33 ± 11.06) years. The mean of OCMI in Group A started to decline directly after 4 days of therapy and went to its lower level after 8 days of therapy, and it was statistically significant (P value <0.05). The change in the mean of OCMI of Group B after 8 days of therapy was also statistically significant (P value <0.05). The difference in the response rates after 4 and 8 days between Group A and B was statistically not significant (P value >0.05). Both groups showed statistically significant prophylactic effect after 1, 2 and 3 months from starting therapy. No significant side effects were noticed in both groups as both oils are edible oils. Conclusion: Sesame and pumpkin seed oils had a statistically significant effective therapeutic and prophylactic action against RAS. No local or systemic side effects were observed during the course of therapy. These two edible oils will give new hope for management of these chronic recurrent oral ulcers.
Keywords: Sesame seed oil, Pumpkin seed oil, Edible oils, Recurrent aphthous stomatitis
Cite this paper: Khalifa E. Sharquie, Adil A. Noaimi, Douaa S. Ahmed, Topical Sesame Seed and Pumpkin Seed Oils have Therapeutic and Prophylactic Role in the Management of Recurrent Aphthous Stomatitis, American Journal of Dermatology and Venereology, Vol. 9 No. 3, 2020, pp. 38-42. doi: 10.5923/j.ajdv.20200903.02.
1. Introduction
- Recurrent aphthous stomatitis (RAS) is one of most common cause of oral ulceration that associated with a major health problem as it affects at least 20% of population all over the world [1]. There are many varieties of RAS like minor, major and herpetiform. Minor ulcers (80%) are less than one centimeter in diameter; usually heal within 2 weeks without scarring. Major ulcers (10%) usually one centimeter or more in diameter, take 10 - 40 days to heal and may leave scars, while herpetiform ulcers (10%) are cluster of dozens of smaller ulcers [2]. There are many theories that have been suggested to explain its etiopathogenesis but the proper cause is still not fully explained [3].The prognosis of this disease could not be predicted, still some patients might get remission either as a result of therapy or spontaneously [4]. A large number of therapies both topical and systemic have been used in treatment of RAS, including topical, intralesional and oral steroid [3], tetracycline, [5] topical honey, [6] lactic acid 5% mouthwash, [7,8] BCG vaccine, [9] nigella sativa oil, [10] oral dapsone and oral zinc sulfate, [11] oral colchicine, [12] oral isotretinoin, [13] oral thalidomide, [14] oral clofazmine [15] and others.Recently, an Iraqi study showed that Pumpkin seed oil has an effective therapeutic and prophylactic effect in management of RAS, as Pumpkin seed oil is rich source of vitamins, minerals and antioxidants, in addition it has good anti-inflammatory action. [16]Sesame oil contains Sesamin (0.4-1.1%), sesamolin (0.3-0.6%) and traces of sesamol that contribute to the unique therapeutic properties of sesame oil. [17] In addition, sesame contains ample amounts of oleic, linoleic, palmitic and stearic acid which together comprise 96% of the total fatty acids. [18]Sesame oil and its lignan sesamol had shown to have potent anti-inflammatory agents as they have an excellent protective effect against endotoxin-associated inflammatory damage because they inhibit the release of inflammatory mediators. Sesamol also inhibits endotoxins from binding to its receptor; thus reduces inflammatory transcription factor NF-κB activation. [19] Sesame oil has also a high content of unsaturated fatty acids (palmitic, stearic, oleic and linoleic acids), well as well presence of lignans (sesamin, asarinin, sesamolin, and sesamol) and gamma-tocopherol. All these compounds may be responsible for the pharmacological activities, since several studies have demonstrated that fatty acids reduce the levels of prostaglandins and leukotrienes. [20] Vitamin E, a fat soluble antioxidant, protects the body from harmful oxidizing compounds. Sesame seed oil contains gamma tocopherols along with sesaminol and sesamin which possesses Vitamin E like activity. [21] So, the aim of the present work is to evaluate the efficacy and prophylactic actions of topical Sesame seed oil in comparison with Pumpkin seed oil in the management of RAS.
2. Patients and Methods
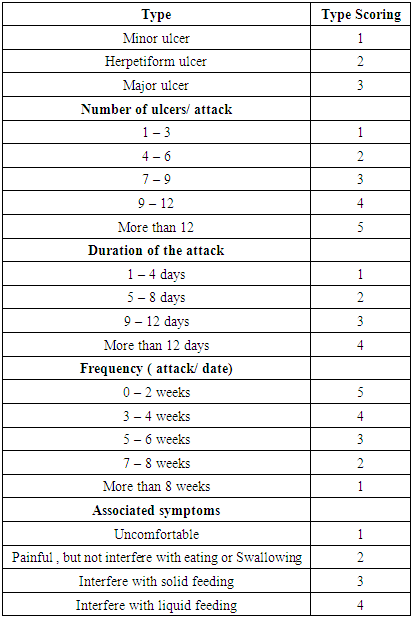
- This is a single blind therapeutic comparative study to evaluate the effectiveness of topical Sesame seed oil in treatment and prophylaxis of RAS in comparison with Pumpkin seed oil. Patients with RAS enrolled in this study were those who attended Baghdad Teaching Hospital - Centre of Dermatology in the period between March 2018 and December 2019.Inclusion criteria: Patients with RAS in the present work were those with early onset ulceration (less than 3 days duration) and had little or no benefit obtained from other conventional therapy in previous attacks. Also they stopped their treatment at least two months before the present therapy. The diagnosis of RAS was based on history and clinical examination. History was obtained regarding age, gender, occupation, past medical history, drug history, smoking and alcohol intake, the recurrence rate and history of the same condition or other illness in the family. Also, they were asked about any aggravating factors including food, stress and trauma or associated symptoms. All patients were fully examined regarding shape, size and number of the lesions. Investigations were done for all patients regarding pathergy test, complete blood picture, ESR and HLA-B51 to exclude patients with Behcet’s disease and other internal causes of oral ulcerations. All patients were seen by ophthalmologists, Neurologist and Rheumatologist whenever needed to exclude findings suggestive for Behcet's disease. Formal consent was taken from each patient and/or their parents before starting the trial after a full explanation for the nature of the disease, causes, prognosis, the drug, the method of treatment, duration of follow up and the possible side effects. The ethical approval was granted from the Scientific Committee of the Scientific Council of Dermatology, Iraqi Board for Medical Specializations. Forty five patients with early onset oral ulcerations were enrolled in this study. The patients were divided into two groups:-Group A: on topical Sesame seed oil and Group B: on topical Pumpkin seed oil.Drug preparation: Both oils were ready made in Iraq-Mosul Factory, EMAD trade mark, kept in a clean and tight container till usage. Patients instructed to use both seeds oils topically using cotton piece and applied to the entire oral mucosa two times daily for 3 months. All patients instructed not take any other drug for their apthous ulcer during the course of the study, and to return if they developed drug side effects. An oral clinical manifestations index (OCMI) [16]. Table (1), for each patient was calculated before and during the therapy to assess the response to treatment.
|
3. Results
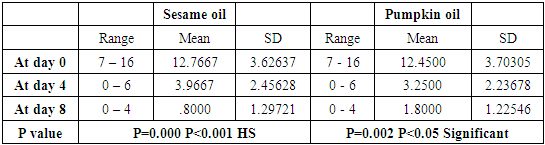
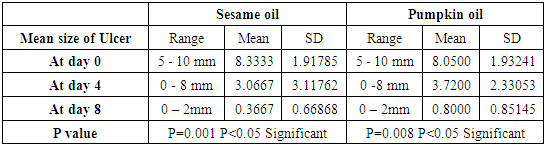
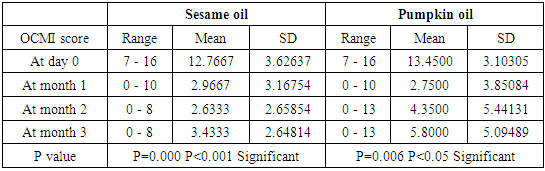
- Forty five patients were enrolled in this study; 30 males (66.6%) and 15 females (33.3%), with male to female ratio was 2: 1. Their ages ranged between 9-60 years with a mean ± SD of 36.33 ± 11.06 years. All investigations for all patients were negative.The therapeutic effect of drugs:► The effect on OCMI scores:Group A (Sesame seed oil): In this group (20 patients), 12 males and 8 females; their ages ranged between 12-60 years with a mean ± SD of 37.75 ± 11.97 years. The OCMI before therapy ranged from 7–16 with a mean ± SD of 12.7 ± 3.6. The mean started to decline significantly to a lower level within 4 days of treatment to be 3.9 ± 2.45. While after 8 days of treatment a significant lower level of data was recorded, the mean was: 0.8 ± 1.2 with a P < 0.001 which was statistically highly significant (Table-2).Group B (Pumpkin seed oil): In this group (25 patients), 18 males and 7 females; their ages ranged between 9-60 years with mean ± SD of 27.48 ± 11.97 years, the OCMI before therapy ranged between 7 and 16 with a mean ± SD 12.4 ± 3.7, the mean started to decline significantly to a lower level within 4 days of treatment to be 3.2 ± 2.2. While after 8 days of treatment a significant lower level of data was recorded, the mean was 1.8 ± 1.2 with a P < 0.05 which was statistically significant (Table-2).
|
|
|
|

|
|
4. Discussion
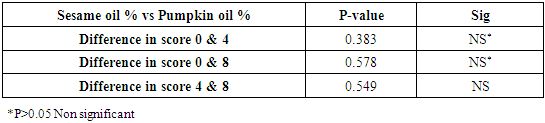
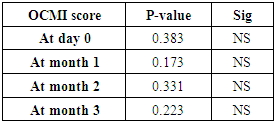
- Despite numerous clinical trials, no medication gives completely reliable cure [4]. A large number of therapies both topical and systemic have been used in treatment of RAS, including topical, intralesional and oral steroid [3], tetracycline, [5] topical honey, [6] lactic acid 5% mouthwash, [7,8] BCG vaccine, [9] nigella sativa oil, [10] oral dapsone and oral zinc sulfate, [11] oral colchicine, [12] oral isotretinoin, [13] oral thalidomide, [14] oral clofazmine [15] and others. Recently, an Iraqi study showed that Pumpkin seed oil has an effective therapeutic and prophylactic effect in management of RAS, as pumpkin seed oil are good source of vitamins, minerals and anti-oxidants, so it has many pharmacological actions like antimicromial, antioxidant and anti-inflammatory effects. [16]This study encouraged us to perform the present work using sesame seed oil to be compared with pumpkin seed oil in management of RAS.Sesame oil contains Sesamin (0.4-1.1%), sesamolin (0.3-0.6%) and traces of sesamol contribute to the unique properties of sesame oil. [17] Also sesame contains ample amounts of oleic, linoleic, palmitic and stearic acid which together comprise 96% of the total fatty acids. [18] These active ingredients have many pharmacological actions mainly anti-inflammatory [18,19] antioxidants [20,21] effects. The results of the present work showed that both therapies are effective as therapeutic and prophylactic agents in controlling RAS.The effect of both therapies on OCMI was statistically significant after 4 and 8 days of therapy and remained statistically significant throughout the three months course of therapy.Sesame seed oil was slightly better than Pumpkin seed oil especially at day8 of therapy and remained better at 2 and 3 months of prophylactic course.No local or systemic side effects were noticed because both oils are edible food.The mechanism of action of sesame seed oil in treatment of RAS cannot be clearly explained, but probable mechanisms of action may be through its anti-inflammatory, [18,19] and antioxidant actions [20,21] which are comparable to actions of pumpkin oil.So in conclusion Sesame seed oil is a safe and effective therapeutic and prophylactic agent in management of RAS and its action was comparable to the effects of pumpkin oil.