-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Dermatology and Venereology
p-ISSN: 2332-8479 e-ISSN: 2332-8487
2019; 8(5): 84-87
doi:10.5923/j.ajdv.20190805.02

Kaposi Sarcoma is Increasing over Years
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKhalifa E. Sharquie1, Adil A. Noaimi1, Salwa F. Taha2
1Department of Dermatology, College of Medicine, University of Baghdad, Iraqi and Arab Board for Dermatology and Venereology, Baghdad Teaching Hospital, Medical City, Baghdad, Iraq
2Dermatology Center, Medical City, Baghdad, Iraq
Correspondence to: Salwa F. Taha, Dermatology Center, Medical City, Baghdad, Iraq.
| Email: |  |
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Kaposi sarcoma (KS) is increasing in Iraq and worldwide. Since the first Gulf War 1990, there was marked increase in cases of classic KS among Iraqi people, in concordance with the rise of incidence of other hematological malignancies. Objective: The aim of the present work is to re-evaluate the current status of KS in Iraq in comparison with the results of the previous Iraqi studies. Patients and Methods: This case series descriptive, clinico-histopathological study was carried out at the Center of Dermatology and Venereology-Medical City, Baghdad, Iraq during the period from October2012 to October 2018. Fifty patients with Kaposi sarcoma were included in this work. A detailed history was obtained from each patient regarding all sociodemographic aspects related to the disease. Full clinical assessment was also carried out. Incisional or excisional biopsy was performed from each patient according to the size and site of the tumor for histopathological confirmation. The following investigations were performed; complete blood picture and erythrocyte sedimentation rate, liver function test, renal function test, chest x-ray, ultrasound of the abdomen, and anti- human immunodeficiency virus (HIV) antibody titer. Results: A total of 50 patients with KS were seen within 6 years. There were 38 males and 12 females with male to female ratio 3.1:1. Their ages ranged from 32-92 (64.55 ± 15.72) years. The duration of the disease ranged from 1-60 (9.02 ± 13.67) months. Sites of predilection were distal extremities in 41(82%) patients. Oral mucosa involvement was seen in only 2(4%) of patients. Palpable lymph nodes were detected in 5(10%) of patients, while visceral involvement was not detected in any patients. The disease was generally asymptomatic in 42 (84%) patients and only 8 (16%) patients presented with slight itching or bleeding from the lesions. The most common type of KS sarcoma was the classic KS in 42(84%) cases followed by iatrogenic KS, 7(14%) cases and HIV related KS in one (2%) patient. The geographical distribution of the patients was as follows: 43(86%) patients were from cities in the middle of Iraq, 4 (8%) patients were from the south of Iraq and 3 (6%) patients were from the north of Iraq. Conclusion: Kaposi sarcoma (KS) is increasing in Iraq. Although the exact cause for the increase is unclear, this could be linked to depleted uranium exposure that was used during the consequent wars in Iraq from 1990 to 2010.
Keywords: Kaposi sarcoma, Iraq
Cite this paper: Khalifa E. Sharquie, Adil A. Noaimi, Salwa F. Taha, Kaposi Sarcoma is Increasing over Years, American Journal of Dermatology and Venereology, Vol. 8 No. 5, 2019, pp. 84-87. doi: 10.5923/j.ajdv.20190805.02.
1. Introduction
- Kaposi sarcoma (KS) is a multifocal, endothelial proliferation predominantly involving the skin [1]. Debate remains as to whether this is a true neoplasm or a reactive process [2]. Human herpes virus (HHV-8) was recognized as the probable inductive agent of all clinical variants of KS [3]. HHV-8 along with genetic, immunological and environmental factors, are closely involved in its pathogenesis [3].Immunohistochemical and ultrastructural studies have firmly established the endothelial nature of KS, but it remains controversial whether this endothelial phenotype is vascular, lymphatic or perhaps a composite of both. Although recent evidence points towards a lymphatic origin [4].There are four distinct clinicopathological subtypes: Classic, African endemic, Iatrogenic and AIDS associated. The most distinguishing clinical features among these subtypes are the rate of progression and the degree of non-cutaneous involvement [1].Classic KS is found mainly in elderly males of Jewish (Ashkenazi) descent and/or of Mediterranean/Eastern European descent. Male: female (M: F) ratio varies from 15:1 (older literature) to 3:1 or 1:1 (more recent observations). [5] It typically presents as slowly growing, pink to redviolet macules on the distal lower extremities that may coalesce to form large plaques or develop into nodules or polypoid tumors. Lymphedema can occur. Involvement of oral mucosa and internal organs is rarely seen [4].In adults, the African endemic form can be locally aggressive in the skin, but is rarely so systemically. The African endemic form in children is typically lymphadenopathic with or without cutaneous involvement and is often fatal within 2 years nodes [1].KS due to iatrogenic immunosuppression is generally clinically similar to classic KS. It may resolve completely upon removal of immunosuppressive therapy [5].KS associated with HIV infection most commonly affects HIV-infected patients with advanced immune impairment and CD4+ T cell counts of fewer than 500 cells per cubic millimeter. The face and oral mucosa are relatively frequently involved. Involvement of lymph nodes, gastrointestinal tract and lungs is common [6].KS was a rarely encountered tumor in Iraq till the first Gulf War 1990, where there was marked increase in cases of classic KS.There are two previous studies regarding KS in Iraq that had been carried out in the same hospital, in Baghdad City. In the first study from 1974-1984, where 21 patients with KS were seen within 10 years [7]. The second study from 1999-2001, showed an upsurge of new cases of Kaposi sarcoma in Iraqi patients, where 20 patients were seen in a period of less than 2 years [8]. Since then, this upsurge of KS continues.Therefore, the aim of the present work is to re-evaluate the current status of KS in Iraq and to compare the result with the previous studies.
2. Patients and Methods
- This case series descriptive, clinical and histopathological study was carried out at the Center of Dermatology and Venereology-Medical City, Baghdad Teaching Hospital, Baghdad-Iraq during the period from October 2012 to October 2018. Fifty patients with Kaposi sarcoma were included in this work.A full history was obtained from each patient regarding all sociodemographic aspects including: age, gender, address, mobile no., previous medical history, marital status and occupation. The age of onset, duration of disease, evolution of lesion, immune suppressive conditions or drugs, family history were also recorded. Full clinical assessment was carried out including: the site, type and distribution of lesions. Leg edema, mucous membranes and lymph nodes were evaluated. The following investigations were performed; complete blood picture and erythrocyte sedimentation rate, liver function test, renal function test, chest x-ray, ultrasound of the abdomen, anti-human immunodeficiency virus (HIV) anti- body titer, and skin biopsies for histopathological evaluation were done for all patients to prove the diagnosis.Formal consent was taken from each patient before starting the study. The aim of the study and the nature, course and prognosis of the disease in addition to available treatment options were fully explained and discussed with the participants. Also, the ethical approval was given by the scientific committee of the Scientific Council of Dermatology and Venereology-Iraqi Board for Medical Specializations. Digital photography was taken using Sony digital, 16.1 megapixel camera in the same place and distance with fixed illumination.SPSS v.22 (statistical package for social sciences version 22) is used for data input and analysis.
3. Results
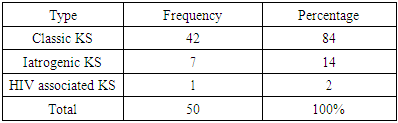
- A total of 50 patients with KS were documented during 6 years. There were 38(76%) males and 12 (24%) females with male to female ratio 3.1:1. Their ages ranged from 32-92 years with a mean ± SD of 64.55 ± 15.72 years and the most common age group affected was 70-80 years.The duration of the disease ranged from 1month to 60 months with a mean ± SD of 9.02 ± 13.67 months.Sites of predilection was distal extremities in 41 (82%) patients, face (dorsum of nose) in one (2%) patient with HIV, penis in one (2%) and generalized distribution in 7 (14%) patients. Oral mucosa involvement was seen in only 2 (4%) patients as violaceous plaques and nodules on hard palate and tongue. Palpable lymph nodes were detected in 5(10%) patients. (Figure 1,2,3)
 | Figure 1. A 40 years old female with HIV associated KS on nose |
 | Figure 2. A 41 years old male with generalized KS 3 months post renal transplantation |
 | Figure 3. A 70 years old female presented with clas- sic KS on lower limbs |
|
4. Discussion
- Kaposi sarcoma was a rarely encountered tumor in Iraq till the first Gulf War 1991, where there was marked increase in cases of classic KS. There are two previous studies regarding KS in Iraq. In the first study from 1974-1984, where 21 patients with KS were seen in a period of 10 years [7]. The second study from 1999-2001, showed an upsurge of new cases of Kaposi's sarcoma in Iraqi patients where 20 patients were seen in a period of less than 2 years [8]. Since then, this upsurge of KS continues and the present study included 50 patients within 6 years in the same medical center.KS occurs worldwide, affecting all races and it is approximately twice as common in men as women. Although old literature revealed a very high male to female ratio (15:1); many recent studies revealed a male to female ratio of (2:1). The present work showed a ratio of (3.1:1) which is comparable with that Al-Waiz et al study (2:1). [8]In this work, patients age range between 32-92 years with predilection for middle aged and older. This is almost consistent with medical literatures. The mean age of patients was 64 years, while in Al-Waiz et al study [8], the mean age was 54 years.Mean duration of the disease was 9 months which is lower than Al-Waiz et al [8] where the mean duration was 19 months.The clinical picture and morphology of the skin lesions in the present study was closely comparable to the 2 previous reports.Regarding the site of predilection, the present work revealed that 82% of patients had their lesions on the distal extremities; 2% of patients had their lesions on face; 2% on penis and 14% of patients had generalized distribution. This result was consistent with the previous work of Al-Waiz et al. [8]Mucosal involvement was detected in 4% of patients, this result was lower than Al-Waiz et al study were mucosal in- volvement were seen in 10% of patients. Palpable regional lymph nodes were detected in 10% of patients, which is similar to Al-Waiz et al study. [8]In present work, visceral involvement was not detected in any patients after full screen work up while in Al-Waiz et al study [8] 20% of patients had visceral involvement.Regarding the geographical distribution of patients, 86% of patients were from the middle of Iraq, while 8% were from the South and 6% were from the North of Iraq. This result was comparable to Al-Waiz et al study [8] where 75% of patients from the middle, 20% from the South and 5% from the North of Iraq.Since the first Gulf War 1990, there was marked increase in cases of classic KS in Iraqi population, in concordance with the rise of incidence of other hematological malignancies. [9,10] The cause of this upsurge is not clear but it could be related to exposure to chemical weapons and depleted uranium during the consequent wars that Iraq had faced since 1990.Further studies is warranted to assess the seroprevalence rates of HHV-8 in Iraqi population and to estimate environmental pollution related to depleted uranium and its impact on heath and increasing cancer incidence in Iraq.
5. Conclusions
- Kaposi’s sarcoma (KS) is increasing in Iraq. Although the exact cause for the increase is unclear, this could be linked to depleted uranium exposure that was used during the consequent wars in Iraq from 1990 to 2010.