-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Dermatology and Venereology
p-ISSN: 2332-8479 e-ISSN: 2332-8487
2019; 8(4): 61-65
doi:10.5923/j.ajdv.20190804.02

Squamous Cell Carcinoma of Lower Lip: Topical Podophyllin is an Alternative Therapy for Early Cases
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKhalifa E. Sharquie1, Wesal K. Al-Janabi2
1Department of Dermatology, College of Medicine, University of Baghdad, Iraqi and Arab Board for Dermatology & Venereology, Baghdad Teaching Hospital, Medical City, Baghdad, Iraq
2Dermatology Center, Medical City, Baghdad, Iraq
Correspondence to: Wesal K. Al-Janabi, Dermatology Center, Medical City, Baghdad, Iraq.
| Email: |  |
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Although surgical excision is the first line of management for squamous carcinoma of lip, patients with early cases without regional lymphadenopathy or distant metastasis refuse surgical intervention and topical therapy should be looked for. The aim of study: Is to analyze the demographic and clinical features and treatment modalities with follow up findings. Patients and methods: Thirty-six cases of biopsy proved primary SCC of the lower lip from the Dermatology Center, Baghdad Medical City, Baghdad, Iraq during the period from January 2006 to April 2019 were included. Twenty-nine patients were considered for surgical management including electric cautery, while seven patients were treated with Podophyllin (25%) weekly sessions for six weeks with follow up of one year. Results: The male-female ratio was 5:1. The mean age was 54.1±17.9 years. Nearly all of them were skin type III and IV. Single nodular vegetating ulcerative lesion was the feature present in 33 patients, while three patients showed, diffuse lower lip involvement simulating Cheilitis. None had regional lymphadenopathy or distant metastasis. Twelve patients had signs of photoaging. Six patients had risk factors like actinic and oral Lichen planus, Porphyria and solar facial Porokeratosis. No recurrence in patients treated with Podophyllin. Conclusion: Squamous carcinoma of lower lip is disease of middle age males that commonly present with single nodular vegetating ulcerative lesions with no local lymphadenopathy or distant metastases. Topical Podophyllin 25% solution should be kept as alternative for early cases especially those who refuse surgical intervention.
Keywords: Squamous cell carcinoma (SCC), Lip, Podophyllin, Iraq
Cite this paper: Khalifa E. Sharquie, Wesal K. Al-Janabi, Squamous Cell Carcinoma of Lower Lip: Topical Podophyllin is an Alternative Therapy for Early Cases, American Journal of Dermatology and Venereology, Vol. 8 No. 4, 2019, pp. 61-65. doi: 10.5923/j.ajdv.20190804.02.
1. Introduction
- The lips are a not uncommon, but often overlooked site for nonmelanoma skin cancers (NMSC), [1]. Lip cancer is the most common malignant lesion of the oral cavity, constituting 25-30% of all oral cavity cancer cases and is the second most common malignancy of the head and neck overall after cutaneous malignancy [2].Unlike other sub-sites of the oral cavity, sun exposure is a well-established risk factor for development of lip cancer. This helps to explain why 90% of lip cancers occur on the lower lip, since it has a higher level of sun exposure compared to the upper lip, which is shielded by the nose and is angled slightly downwards. There is also a pronounced geographic variability in incidence, which is consistent with sun exposure patterns. Thirty percent of patients with lip cancer have outdoor occupations. Tobacco use, including dip, alcohol use and immunosuppression are also risk factors. HPV has been associated with lip malignancy, but its role in the pathogenesis of the disease is not as defined as with other sub-sites in the oral cavity and oropharynx [2]. Tanning beds, exposure to coal tar, arsenic compounds, radiation, and hot dry dessert like climate and burn sites are also other risk factors [3].Lip cancer is mostly seen in male patients [1] in their 6th decade of life and with fair complexions [1,2].Nearly 30% of all squamous cell carcinomas affect the lip [1].Lower lip cancers in 90% are squamous cell type [2,4] that involve the vermillion, whereas upper lip cancer is usually basal cell type, and arise from the lip skin rather than vermillion area. There is a high incidence of a second primary skin malignancy in patients with lip carcinoma due to the common sun exposure risk. [2] SCC of the lip develops from actinic damage, with 95% of the cases involving the lower lip [5]. It occurs most frequently in male patients (male-female ratio, 6:1), [6], aged 50 years or over who have been exposed to sunlight for long periods. As with other malignant tumors, tobacco and alcohol abuse also play a role, as possible triggers. The tumor is very rare in younger patients, yet it has been reported in patients receiving immunosuppressive therapy after renal transplant [6,7]. There is concern about an ongoing increase in younger patients and in women. More than one in 10 cases is now diagnosed in people below age 50 [1]. SCC of lower lip is more aggressive than conventional squamous cell carcinoma affecting other body regions [3].The typical picture of SCC of the lower lip is of an ulcerated lesion with raised margins. It may appear in any part of the lower lip, yet the lateral and central portions are most commonly involved. The upper lip is less frequently committed; however, when it is, by far more aggressive than carcinoma of the lower lip. Although the ulcerative presentation is most common, other expressions, such as exophytic lesions with apparently limited margins, may also appear. In some cases after biopsy of the lesion, rapid local recurrence may occur, involving a greater portion of the lip [7].As it on highly visible location, the majority of lip cancers are easily detectable and treatable at an early stage. The most commonly employed treatments include surgery, radiation, and Cryotherapy using freezing with liquid nitrogen, with cure rates for early lesions nearing 100 percent [4]. Although cancers of the lip have relatively low rates of spread to nearby lymph nodes and distant sites, the relapse rate after treatment can range from 5-35 percent. Once these cancers spread to local lymph nodes, five-year survival rates decrease to approximately 50 percent [8].Podophyllin is an alcoholic plant extract obtained from dried rhizomes of common plants called emodi (Indian Podophyllum) or Podophyllum peltatum (May apple or Mandrake). Podophyllum resin contains many active ingredients that work through multiple actions mainly by arresting mitosis and differentiation, blocking oxidation enzymes in Tricarboxylic acid cycle and thus interfering with cell nutrition, inhibiting axonal transport, protein, RNA, and DNA synthesis and affecting mitochondrial activity with reducing cytochrome oxidase activity [9]. Podophyllin had been used over a long time for the treatment of viral warts [9], and is indicated for the treatment of Condyloma Acuminatum ,venereal warts [10], with report of use in genital warts in infants [11] oral hairy leukoplakia, [12], juvenile papilloma of the larynx, [13] and Molluscum Contagiosum [14]. Podophyllin 25% in benzoin co had been used as effective therapy for cutaneous leishmaniasis [15], basal cell carcinoma [16], actinic keratosis [17], facial angiofibroma in tuberous sclerosis [18] and localized plaque psoriasis [19].The aim of the present study is to analyze demographic and clinical features, associated risk factors and treatment modalities with follow up findings of a series of patients diagnosed with primary SCC of the lip.
2. Patients and Methods
- This study of 36 cases of primary SCC of the lower lip was conducted at the Dermatology Center, Baghdad Medical City, Baghdad, Iraq during the period from January 2006 to April 2019. All the cases of cancer of the lower lip, over the past 13 years were collected and evaluated for the demographic data like age, gender, occupation including outdoor activity. Associated risk factors like alcohol drinking and smoking were reviewed. Clinical features as location of the tumor on lip, the type of the lesion, cervical metastasis at presentation, in addition to compete systemic evaluation. Incisional biopsy with histological sections stained with Hematoxylin and Eosin (H&E) results were retrieved and assessed. Treatment modalities with follow up findings were also reviewed. Twenty-nine patients (80.5%) were considered for surgical therapy including electrical diathermy. Seven (19.5%) patients were treated with topical Podophyllin (25%) weekly sessions for six weeks with follow up period of one year. Topical Podophyllin 25% was prepared by mixing 25g of Podophyllum resin in tincture benzoin. The patient once weekly for six weeks applied the Podophyllin. Pre, during and post treatment photographs were taken for efficacy evaluation and follow up. Data entry followed by inferential statistics were carried out by the researchers using the software statistical package for social sciences (SPSS) version 20. Continuos variables presented as mean ±SD (Standard deviation) and discrete variables as numbers and percentages.
3. Results
- Thirty-six patients with SCC of the lower lip were studied and evaluated; 30 (83.3%) patients were males and six (16.6%) patients were females with male-female ratio of 5:1. All of patients came from urban rather than rural zones. Their ages ranged between 14-80 years with a mean± SD was 54.1±17.9 years. Nineteen (52.7%) of patients were over 60 years. All of them had outdoor activities. The duration of disease was less than a year in all the patients. None of patients gave history of smoking or alcohol drink. All of them were skin type III and IV except one with fair skin and blue eyes. Histopathological evaluation of biopsies showed features of squamous cell carcinoma including invasion of dermis by abnormal keratinocytes (hyperchromatic, pleomorphic, epithelioid) with many keratin Pearls, squamous eddies, acantholysis and pseudoglandular pattern and lichenoid infiltrate. (Fig.1). Single nodular vegetating ulcerative lesion was the most common feature present in 33 (91.66%) patients with overlying crustation and granulation tissue (Fig.2). The lesion involved the middle portion of lip in 18 (50%) (Fig. 2), the right side in 7 (19.4%), the left side in 7 (19.4%) patients and on right commissure in only one patient. while 3 (8.3%) patients showed diffuse lower lip involvement simulating cheilitis (Fig. 3). No regional lymphadenopathy was found in any patient and no one presented with evidence of distant metastasis. Twelve patients (33.3%), 11 (91.6%) males and 1 (8.3%) female, had signs of photoaging as erythema, telangiectasia, lentigines, actinic keratosis and wrinkles. Six (16.66) patients had associated risk factors like two (5.5%) male patients had facial actinic lichen planus while other two (5.5%) (One male and one female) had oral lichen planus of lip and tongue (Fig. 4); one (2.7%) male child had porphyria and one (2.7%) male patient with solar facial porokeratosis (Fig.5). Twenty-nine patients (80.5%) were considered for surgical therapy including electrical diathermy. Seven (19.5%) patients were treated with topical Podophyllin (25%) weekly sessions for six weeks and all lesions showed complete clearance, without recurrence over follow up period of one year (Fig. 6).
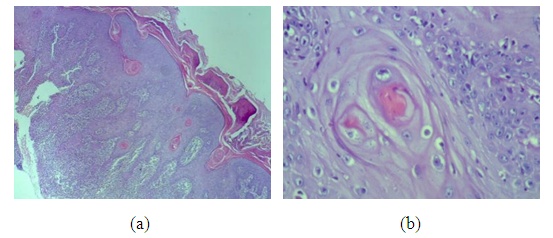 | Figure 1. (a) H& E stain × 40; (b) H& E stain × 400. The histopathology of a well-differentiated SCC of lower lip in 60 years old male patient showing invasion of dermis by abnormal keratinocytes with many keratin Pearls, squamous eddies and lichenoid infiltrate |
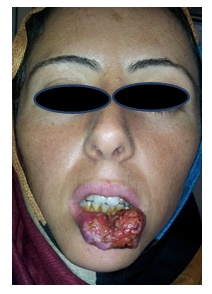 | Figure 2. Thirty-five years female patient with the nodular vegetating ulcerative lesion |
 | Figure 3. SCC in 85 years male patient with actinic Chielitis like diffuse lip swelling |
 | Figure 4. SCC of lower lip in 43 years male patients with lichen planus |
 | Figure 5. Thirty years male patient with facial solar porokeratosis of nose with lower lip SCC |
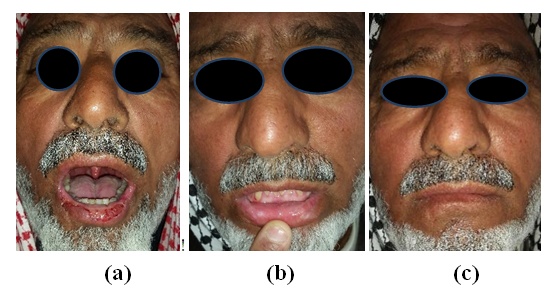 | Figure 6. Sixty years male patient with diffuse SCC of lower lip. (a) Before treatment with topical 25% Podophyllin weekly sessions. (b, c) After treatment with clearance at one year follow up |
4. Discussion
- Skin cancer whether NMSC, melanoma or other types were used to be seen relatively rarely in Iraqi population [20], but after American’s invasion in 1991; there was an upsurge of new cases, including Kaposi Sarcoma [21], Malignant Melanoma [22], Dermatofibrosarcoma protuberance [23] and Mycosis Fungoides [24]. Basal Cell Carcinoma in Iraq is much more common than SCC as in other parts of the world [25].Although SCC of the lower lip is relatively a rare problem, but it was also noticed to be increased with surprisingly no obvious predisposing lesions other than actinic damage. The present work described 36 cases of lower lip SCC over the last 13 years with comparable age (52.7% over 60 years) [26] and gender male predominance, 83.3% as compared to previous reports [26]. In the last twenty years, there was a chiasm in population sector whether rural or urban as many rural people moved to cities. Therefore, a larger percentage of patients came from urban areas similar to previous reports [26] unlike what is described in some other studies [27]. Iraq climate is sunny nearly over the year, so most people considered to have outdoor activities. Hence, the common risk factor was excessive daily sunlight exposure as 30 (83.3%) patients were males with outdoor activity. Most of patients were dark skinned except one with fair skin and blue eyes unlike previous reports being mostly in white persons [27]. Bad oral hygiene and smoking used to be claimed as a trigger [28], but this observation was not confirmed in the present study.Single nodular vegetating ulcerative lesion was the feature present in 33(91.66%) patients with overlying crustation and granulation tissue which is comparable with findings reported by other studies [7,26]. In the present work, no regional lymphadenopathy was detected, but proved to be present by other studies [26].Twelve patients (33.3%), 11(91.6%) males and 1(8.3%) female, had signs of photoaging as erythema, telangiectasia, lentigines and wrinkles, while six cases (16.6%) had preexisting skin diseases as a risk factors: two patients with Lichen planus actinicus, other two with oral Lichen planus of tongue, one with Porphyria and one with solar facial Porokeratosis. Solar facial Porokeratosis was not uncommonly seen on the face of Iraqi young female patients around the nose but no association with SCC had been reported SCC [29].Fortunately, lip cancer remains one of the curable malignancies in the head and neck. The 10-year cause specific survival can be as high as 98% and recurrence free survival is greater than 90%. This is mainly because the lips are prominently located and allow for early detection and treatment of lesions. Tumors that are neglected may portend a worse prognosis and progressively involve the skin of the mentum, alveolar mucosa, and mandible, floor of mouth, and tongue, as well as local regional nodal and distant metastasis [2].Surgery including excision and or diathermy is always indicated as the most effective curative technique for lip carcinoma. Still some patients might refuse surgery especially early cases and in this situation, an alternative therapy should be looked for. Topical Podophyllin has been assessed as alternative effective therapy for many skin diseases including skin cancers like solar keratosis [17], Keratoacanthoma [30] and Basal Cell Carcinoma [16]. In the present study, seven cases (19.5%) of lower lip SCC were treated with 25% Podophyllin once weekly application and the results were encouraging as complete clearance of lesion was seen and no relapse for up to one-year follow up. The mechanisms of action of Podophyllin includes arresting mitosis and differentiation and clearance of cancer through its different therapeutic antineoplastic actions [9]. Accordingly topical Podophyllin should be kept as alternative choice of therapy for SCC of lip especially in early cases.
5. Conclusions
- Squamous cell carcinoma of lower lips is not uncommon increasingly seen tumor of middle age males that commonly present with single nodular vegetating ulcerative lesion with no local lymphadenopathy or distant metastases. Preexisting risk factors were observed in only 16.66% of cases; Topical Podophyllin therapy should be kept as alternative therapy for early cases especially in patients who refuse surgery.