Hayder R. M. Al-Hamamy 1, Basman M. Fadheel 1, Hadeel J. Hasan 2
1Departments of Dermatology, College of Medicine, University of Baghdad, Iraq
2Department of Dermatology, Baghdad Teaching Hospital, Medical City, Baghdad, Iraq
Correspondence to: Basman M. Fadheel , Departments of Dermatology, College of Medicine, University of Baghdad, Iraq.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Background: The breast has a great aesthetic importance .It is also the site of the most common malignancy in females. Diagnosis of the diseases affecting the breast sometimes poses difficulties. Objectives: To determine the frequency and clinical features of dermatoses affecting the female breast in referred patients to Dermatology department of medical city teaching hospital. Patients and methods: The study is an outpatient hospital based descriptive study. It was conducted at the Department of dermatology -Baghdad Teaching Hospital in Baghdad during one year period from October 2014-October 2015. Any female patient with cutaneous lesion primarily involving the breast referred to the center was included in this study. Full clinical skin examination of skin lesion and general dermatological examination was performed. Results: A total of 92 female patients were included in the study. Their ages ranged from (13-70) years, mean age 38.38 years SD± 14.67. The most common inflamatory skin disease was atopic dermatitis. It was diagnosed in 15 patients (15.21%). Malignant tumors of the breast were diagnosed in 17 patients (18.47%). Metastatic breast cancers were confirmed by biopsy in 9 patients. Paget's disease was diagnosed in 3 patients. Conclusions: Breast cancer is the most common diagnosis in the patients referred to the department which stresses the early detection of this cancer. Atopic dermatitis is a common entity.
Keywords:
Dermatoses, Breast
Cite this paper: Hayder R. M. Al-Hamamy , Basman M. Fadheel , Hadeel J. Hasan , Frequency and Clinical Features of Dermatoses Affecting the Breast Area in Iraqi Women, American Journal of Dermatology and Venereology, Vol. 5 No. 3, 2016, pp. 46-50. doi: 10.5923/j.ajdv.20160503.02.
1. Introduction
The breast is comprised of three major structures: skin, subcutaneous tissue, and breast tissue, with the last comprising both parenchyma and stroma. [1]The parenchyma is divided into 15 to 20 segments that converge at the nipple in a radial arrangement. The collecting ducts that drain each segment are 2 mm in diameter, with sub areolar lactiferous sinuses of 5 to 8 mm in diameter. Approximately 10 major collecting milk ducts open at the nipple. [1, 2]Cyclic changes in the sex steroid hormone levels during the menstrual cycle profoundly influence breast morphology. Under the influence of follicle-stimulating hormone and luteinizing hormone during the follicular phase of the menstrual cycle, increasing levels of estrogen secreted by the ovarian Graafian follicles stimulate breast epithelial proliferation. Progesterone induce changes in the mammary epithelium during the luteal phase of the ovulatory cycles. [3]Breast infection in lactating mothers is a common entity which in the majority of cases can be explained by ascending infections. However, it has been noticed that the number of non-lactating women presenting with breast abscesses is rising. The distinction between mastitis and frank abscess is of great importance since the management of these two entities varies from antibiotics to drainage either by aspiration or incisions. [4] Fungal infections of the breast are generally uncommon. Candida albicans is the exception, being quite common. Candida intertrigo in the inframammary area is the more common presentation of candidiasis, but Candida can involve the nipple or areola as well. Candida intertrigo presents with beefy erythema often in association with satellite papules and pustules, pruritus, and maceration in, and adjacent to, the inframammary fold. Predisposing factors include obesity, diabetes, and pendulous breasts. However, any condition that creates a warm moist environment may lead to the development of intertrigo. [2, 5]Dermatitis of the breast and/or nipple is quite common, Nipple eczema represents the most common presentation of atopic dermatitis of the breast. Although it is not a specific indicator of disease, it is so common as to be considered a minor criterion in the diagnosis of atopic dermatitis. [6] Nipple dermatitis can often present during breastfeeding. Typically this occurs secondary to the feeding action of the infant. However, when solid foods are introduced, some women may react to allergens in the food residue in the infant’s mouth. [7] Psoriasis may affect any area of the breast. In the inframammary area it generally appears as a well demarcated, pink plaque that often appears moist and has minimal or no scale .When psoriasis occurs on other areas of the breast, it tends to present similarly to its presentation elsewhere on the body. [8] Carcinoma of the breast is the most common cancer and the second most common cause of death in women. [9] Breast cancer is classified as noninvasive (in situ) or invasive .In situ lesions are further classified into lobular carcinoma in situ (LCIS) and ductal carcinoma in situ (DCIS). [10] The skin changes associated with invasive breast cancer include skin retraction, as well as the inflammatory changes characteristic of inflammatory breast cancer. Skin retraction may manifest as shallow or deep skin dimples, or as shrinkage of the entire breast. It occurs when the invasive cancer becomes attached to a suspensory ligament (Cooper’s ligament) with subsequent fibrosis and shortening of the ligaments. [11] More advanced skin changes include edema and ulceration. [12] Paget's disease of the breast, a disorder of the nipple–areola complex, is an uncommon disease, accounting for 1–4.3% of all the breast carcinomas. It is often associated with underlying ductal carcinoma in situ and/or invasive ductal cancer. It occurs most commonly in post-menopausal women, often during the sixth decade of life (mean age 57 years), but it has been observed in adolescents and in elderly patients also [13] Objectively, eczematoid changes of the nipple-areola complex are common. The later stages of Paget's disease of the breast are characterized by ulceration and destruction of the nipple-areola complex. [14] The BCC of the breast is believed to be more aggressive than BCC reported elsewhere in the body. [15] Sarcoma and primary lymphoma of the breast are rare and each typically presents as a painless, enlarging mass. [16] Metastasis to the breast may arise from extramammary or mammary malignancies. [17, 18]Hence, the aim of the present study is to determine the frequency and clinical features of dermatoses affecting the female breast in referred patients to Dermatology department of Baghdad Teaching Hospital.
2. Patients and Methods
The study is an outpatient hospital based descriptive study. It was conducted at the Department of Dermatology -Baghdad Teaching Hospital in Baghdad during a one year period from October 2014-October 2015. Any female patient with cutaneous lesions primarily involving the breast referred to the center was included in the study. History was taken including: age, marital status, breast feeding, history and duration of the disease, any associated symptoms, general medical history, personal and family history of any breast disease especially malignancy.Full clinical examination was performed. It included identifying the primary skin lesion with dermatological description, size, site (i.e nipple, areola or other breast skin), any associated tenderness, nipple discharge, palpable breast mass and axillary lymph nodes. The contralateral breast was examined in a similar way followed by complete dermatological examination of the body including scalp, nail and mucous membranes. There were no exclusion criteria in this study and the limitations of this study were, it included patients referred to one center only and relatively small sample size. For patients with clinical presentation suggestive of malignancy incisional biopsy was done and stained by Hematoxyline and Eiosin stain for histopatholgical examination. Patients in whom cancer was diagnosed, referral to the oncology department was done for further management. For patients with suspected fungal infection, scraping of lesion and KOH examination were done and the patients were treated accordingly. Descriptive statistics were calculated by means of computer program Microsoft Word 2010. Range, means, Standard deviation were calculated.
3. Results
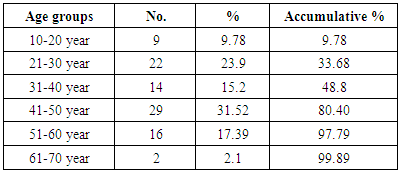
A total of 92 female patients were included in the study. Their ages range from (13-70) years, mean age 38.38 years SD± 14.67. The patients were categorized into 6 age groups. Nine patients (9.78%) with in the age group (10_20) years, 22patients (23%) were in the age group (21-30) years, 14 patients (15.2%) were within the group of (31-40) years. The highest number of patients was in the age group (41-50) year which was 29 (31.52%). Sixteen patients (17.3%) in the age group (51-60). The lowest number was in the age group (61-70) years which was 2 patients (2.1%), (Table 1).Table 1. Age distribution of skin diseases affecting female breast
 |
| |
|
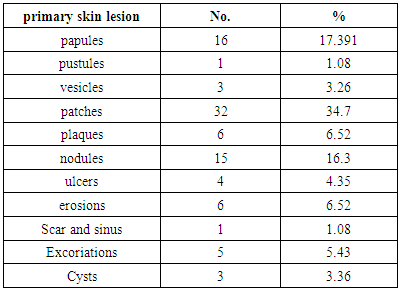
Of the total patients, 9 patients (9.78%) were single while 83 patients (90%) were married. Five married patients (6.02%) were lactating at time of presentation, 78 (93.9%) were non-lactating.During examination the primary skin lesion for each patient was described, 16 patients (17.3%) presented with papules, 1patient(1.01%) presented with pustules, 3 patients (3.23%) had vesicles, 32of the patients (34.7%) presented with erythematous scaly patches which were the commonest, six patients(6.52%) presented with plaques, 15patients (16.3%) had nodules, 4 patient presented with ulcer while 6 patients (6.5%).Presented with erosions, one patients (1%) presented with scars and sinuses, 5 patients (3.2%) presented with excoriations, 3 patients (3.36%) presented with cystic lesions (Table 2).Table 2. The primary skin lesion of diseases affecting female breast
 |
| |
|
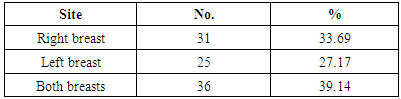
Thirty one patients (33.69%) had skin lesions in the right breast while 25 (27.17%) had Left breast lesions. Thirty-six (39.14%) patients had lesions in both breasts (Table 3).Table 3. Patients categorization according to the site of involvement of skin diseases affecting female breast
 |
| |
|
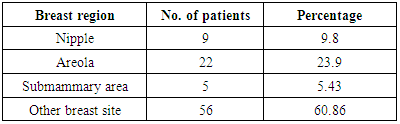
During examination 9 (9.8%) patients had skin lesions involving the nipple mainly, 22 patients (23.91%) having skin lesions involving the areola, 5 (5.43%) patients had submammary lesions and 56 patients (60.8%) having skin lesions involving other parts of the breast. (Table 4)Table 4. Patients distribution according to region mainly involved
 |
| |
|
The skin diseases classified according to frequencies shown in table 5.Table 5. Frequency of skin diseases involving the breast
 |
| |
|
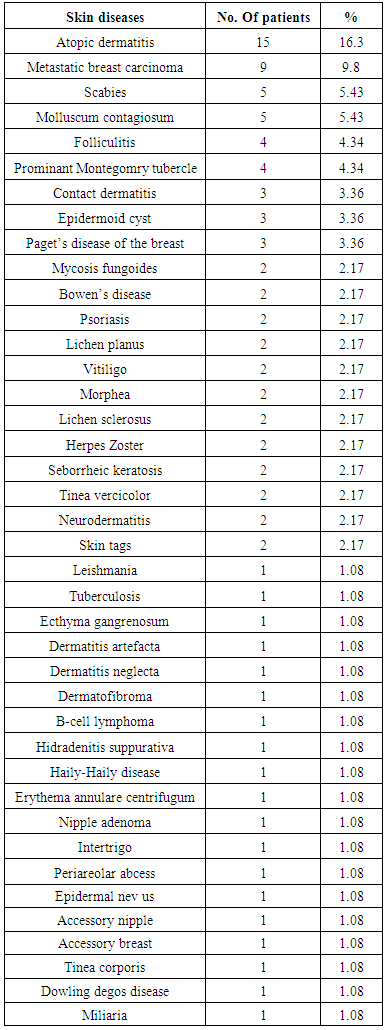
The most common skin disease was atopic dermatitis which was diagnosed in 15 patients (15.21%). The site of involvement was the nipple and areola (table 6). Intensely itchy patches were evident on clinical examination, and they responded to topical steroid with emollients. Malignant tumors of the breast were diagnosed in 17 patients. Metastatic breast cancer was confirmed by biopsy in 9 patients. Seven patients had lesions on the same side of a previous mastectomy for breast cancer followed by chemotherapy. The lesions were painless infiltrative nodules in 6 patients while they were in the shape of scaly erythematous plaque in one patient .Of the other two patients; one patient had history of left mastectomy for breast cancer 2 years ago and she presented with new onset skin lesion on the right breast. The lesions were eythematous plaques and grouped heamrrhagic vesicles. Biopsy showed metastatic breast carcinoma. The other patient presented with breast mass and non-healing ulcer for 1 year duration. Of the other malignant diseases Paget's disease was diagnosed in 3 patients, one patient presented with non- healing nipple ulcer while the other 2 patients presented with dermatitis -like features. Two patients (2.17%) presented with poikiloderma involving both breasts. Mycosis fungoides was diagnosed by biopsy in both patients.One patient with history of systemic large B-cell lymphoma on chemotherapy and presented with violaceous infiltrative plaque on the right breast, biopsy was done and the result was consistent with cutaneous lymphoma. Of the other diseases that were diagnosed in our patients, Molluscum Contagiosum and scabies were diagnosed in 5 patients (5.43%). (Table 5)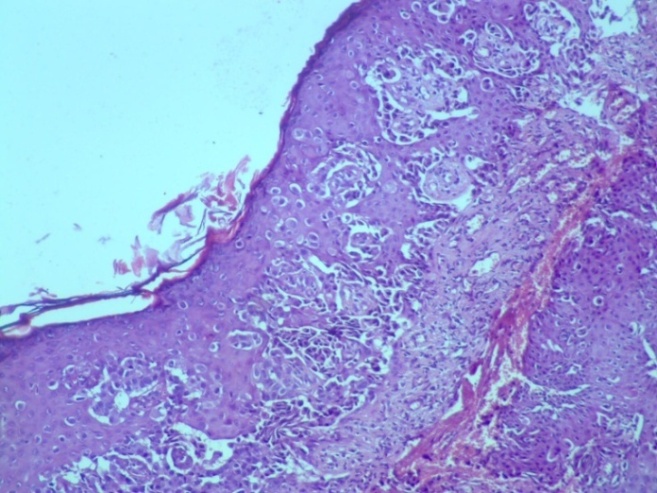 | Figure 1. Histopathology of Paget’s disease on H&E stain showed Pagetoid spread of malignant cells over the entire epidermis |
 | Figure 2. Paget 's disease of the nipple in 48 year old patient |
 | Figure 3. Zosteriform metastatic breast carcinoma of the Right breast in 50 years old patients, she had history of left mastectomy before 2 years |
 | Figure 4. H&E stain of biopsy of the previous patient shows infiltration of the dermis by bizarre shape malignant cells & frequent mitosis |
 | Figure 5. Irritant contact dermatitis from brassière in 35 yr. old patient, 10 days duration |
4. Discussion
The female breast has special importance in examination of the skin integument in any patient due to many factors; Breast cancer is the most common malignancy in females [19] and many cases of breast cancer present with skin involvement; the breast also has a great aesthetic importance [20]; the shape and the skin of the breast has a great value for the patients; the breast has area of modified skin (the nipple and areola) which may sometimes cause diagnostic difficulties for the dermatologist because skin diseases present differently in these areas. In the present study problematic cases were referred to our department for evaluation. Atopic dermatitis was the most common diagnosis in these patients. This may be related to unusual presentation of the disease with primarily involvement of the breast area, or it reflect the awareness of dermatologist of the entity of Paget’s disease which present with eczema -like lesion in the breast. Malignant diseases were diagnosed in 17 patients and metastatic breast cancer to the skin were diagnosed in 9 patients. The treating physicians suspected malignancy because of the infiltrative nature of the skin lesion or because the lesions were refractory to treatment, that is why they referred the patients to our department for further evaluation and follow up. This awareness to breast cancer cannot be overemphasized as the breast cancer remain the first malignancy in female. [19] Scabies remain problematic in our community [21] and its diagnosis is sometimes missed especially if it is confined to one area such as the breast .It is interesting to note that some times normal variant such as prominent Montegomry tubercle cases of confusion .Molluscum contagiosum and its treatment are sometime of concern to both patient and physician .Several treatment are offered such as KOH 10%, immiquimoid cream. [22] It was diagnosed in 5 patients. Other unusual diseases or disease presentation such as Tuberculosis, ecthyma gangrenosum, dermatitis artefacta was seen. Of interest is the diagnosis of dermatitis neglecta in one patient.
References
| [1] | Moffat DF, Going JJ. Three dimensional anatomy of complete duct systems in human breast: pathological and developmental implications. J Clin Pathol 1996; 49: 48. |
| [2] | Lin WW, Karin M. A cytokine-mediated link between innate immunity, inflammation, and cancer. J Clin Invest 2007; 117(5): 1175–1183. |
| [3] | Wittliff JL, Lewko WM, Park DC, et al. Hormones, receptors and breast cancer. In: McGuire WL, ed. Steroid binding proteins of mammary tissues and their clinical significance in breast cancer, vol.10. New York: Raven 1978:327. |
| [4] | Maha S.A AbdelHadi, MD, FACS and Huda A. Bukharie, ABIM†,. BREAST INFECTIONS IN NON-LACTATING WOMEN, .J Family Community Med. 2005 Sep-Dec; 12(3): 133–137. |
| [5] | Opri F. Mammary mycoses. Chemotherapy 1982; 28(Suppl): 615. |
| [6] | William D. james, Timothy G. Berger, Dirk M. Eliston. Andrew's Diseases OF THE Skin Clinical Dermatology. atopic dermatitis, eczema & non infectious immune disorders2012; 5:72. |
| [7] | Amir L. Eczema of the nipple and breast:a case report. J Hum Lact 1993; 9: 173-5. |
| [8] | D. L. Whitaker-Worth, MD, aV. Carlone, MD, aW. S. Susser, MD, et al. Dermatologic diseases of the breast and nipple. J Am Acad Dermatol 2000;43:733-51 |
| [9] | Phillips M, Balducci L. Current management of breast cancer. Am Fam Physician 1996; 53: 657-65. |
| [10] | Sainsbury J, Anderson T, Morgan D, Dixon J. Breast cancer.Br Med J 1994; 309:1150-3. |
| [11] | Wilms J, Schneiderman H, Algranati P. Physical diagnosis: bedside evaluation of diagnosis and function. Baltimore: Williams & Wilkins; 1994. |
| [12] | L. Whitaker-Worth L, Carlone A, et al.. Dermatologic diseases of the breast and nipple D. J Am Acad Dermatol 2000; 43: 733-51. |
| [13] | Karakas C,. Paget's disease of the breast. J Carcinog. 2011; 10: 31. |
| [14] | Sakorafas G, Blanchard K, Sarr M, Farley D. Paget's disease of the breast. Cancer Treat Rev. 2001; 27(1): 9-18. |
| [15] | Sharma A, Ramesh M., Singh A, 1 and Dayananda S. Basal cell carcinoma of the nipple areola complex. J Midlife Health. 2011; 2(2): 89–90. |
| [16] | Ariad S, Lewis D, Cohen R, Bezwoda W. Breast lymphoma: a clinical and pathological review and 10-year treatment results. S Afr Med J 1995; 85: 85-9. |
| [17] | Cecchi R, Brunetti L, Bartoli L, Pavesi M, Giomi A. Zosteriform skin metastases from breast carcinoma in association with herpes zoster [letter]. Int J dermatol 1998; 37: 476-7. |
| [18] | Schwartz RA. cutaneous metastatic disease. J Am Acad dermatol 1995; 33; 161-82. |
| [19] | Lindsey A. Torre, MSPH; Freddie Bray, PhD; RebeccaL. Siegel, MPH; Jacques Ferlay, ME, et al. Global Cancer Statistics, 2012. CACANCER J CLIN 2015; 65:87–108. |
| [20] | Min Soon Kim, Juliano C. Sbalchiero, Gregory P. Reece, et al. Assement of breast aesthetic. Plast Reconstrct Surg. Auther manuscript; 2011 May 19. |
| [21] | Alsamarai AM. Frequency of scabies in Iraq: survey in a dermatology clinic.J Infect Dev Ctries. 2009 Dec 15; 3(10): 789-93. |
| [22] | Metkar A, Pande S, Khopkar U. An open, nonrandomized, comparative study of imiquimod 5% cream versus 10% potassium hydroxide solution in the treatment of molluscum contagiosum. Indian J Dermatol Venereol Leprol. 2008 Nov-Dec; 74(6): 614-8. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML