-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Dermatology and Venereology
2016; 5(1): 1-3
doi:10.5923/j.ajdv.20160501.01

Clinicoepidemiological Study of Bacterial Cutaneous Manifestations of Diabetes Mellitus in Jabir Abu Eliz Diabetic Centre Outpatient Clinic, Khartoum, Sudan
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLOsman Abdel Malik Elbashir 1, Yousif M. Kordofani 1, Abdel Rahman M. Ramadan 2, Abdel Khalig Muddathir 3, Anilkumar Mithani 1, Gamal O. Elhassan 4, 5, Intisar A. Bashir 6, Khalid O. Alfarouk 6, Adil Bashir 7
1Faculty of Medicine, University of Bahri, Bahri, Sudan
2Faculty of Dentistry, Taibah University, El- Madinah El-Munawarah, KSA
3Faculty of Pharmacy, University of Khartoum, Khartoum, Sudan
4Unaizah College of Pharmacy, Qassim University, Qassim, KSA
5Faculty of Pharmacy, Omdurman Islamic University, Omdurman, Sudan
6Faculty of Pharmacy, AL-Neelain University, Khartoum, Sudan
7Institute of Endemic Diseases, University of Khartoum, Khartoum, Sudan
Correspondence to: Adil Bashir , Institute of Endemic Diseases, University of Khartoum, Khartoum, Sudan.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Introduction: Diabetes mellitus, DM, is a group of metabolic disorders with one common manifestation, which is hyperglycemia. Chronic hyperglycemia causes damage to skin, eye, kidney nerves, heart and blood vessels [1]. Objective: To identify the prevalence of common Bacterial Infections in Diabetic patients attending, anoutpatient clinic in JDC, in Khartoum City. Patients and Methods: The design was based on clinical studies, i.e. descriptive. Results: This study revealed that 3.6% of the diabetic patients examined have Bacterial cutaneous infections (BCI); most of them were males (56%), and 56% of the BCI patients are in the age group 40- 65 yrs. Old and 69.3% are married. Most of them are of Northern Sudanese origin (66.4%). BCI are common among housewives and retired men; approximately 66%. Those with the secondary school educational background represented 30.7%. Most patients are of type II DM (82.66%); they had the disease for duration of one year or more (90.7%). Most patients were on adiet, plus oral hypoglycemic drugs (66.3%). Bacterial infections represented 25.7% (furuncles alone were 21.5%). Conclusions: Of the 4398 cases of diabetes mellitus examined for Bacterial cutaneous findings, only 150 diabetic patients (3.6%) showed Bacterial cutaneous lesions.
Keywords: Bacterial Cutaneous Manifestations of Diabetes Mellitus, prevalence, Jaber Abu Eliz diabetic Center (JDC) in Khartoum City
Cite this paper: Osman Abdel Malik Elbashir , Yousif M. Kordofani , Abdel Rahman M. Ramadan , Abdel Khalig Muddathir , Anilkumar Mithani , Gamal O. Elhassan , Intisar A. Bashir , Khalid O. Alfarouk , Adil Bashir , Clinicoepidemiological Study of Bacterial Cutaneous Manifestations of Diabetes Mellitus in Jabir Abu Eliz Diabetic Centre Outpatient Clinic, Khartoum, Sudan, American Journal of Dermatology and Venereology, Vol. 5 No. 1, 2016, pp. 1-3. doi: 10.5923/j.ajdv.20160501.01.
Article Outline
1. Introduction
- Diabetes mellitus, DM, is a group of metabolic disorders with one common manifestation being hyperglycemia. Chronic hyperglycemia causes damage to skin, eye, kidney nerves, heart and blood vessels. The etiology and pathophysiology leading to hyperglycemia, however, are markedly different among patients with DM; dictating different prevention strategies, diagnostic screening methods, and treatment [1]. In June (1997) an international expert committee released a report with new recommendations for the classification and diagnosis of diabetes mellitus [2]. Type 1, type 2, other specific types & gestational diabetes. Arabic numerals are specifically used in the new system to minimize the occasional confusion of type II as the number II [3].Classification of Bacterial Cutaneous infections in diabetes mellitus [5-7]:1. Staphylococcus aureus (Furuncles, carbuncles, and Styes).2. Pseudomonas (Cellulitis, Ostiitis, Cranial nerve damage, Meningitis).3. Non-Clostridial gas gangrenes (E. coli, Klebsiella, Pseudomonas, and Bacteroids).
2. Purpose of the Study
- To identify the prevalence of common bacterial Infections in Diabetic patients attending, anoutpatient clinic in JDC, in Khartoum City.
3. Patients and Methods
- Saturdays, Mondays, and Wednesdays were chosen for data collection, due to the availability of the different specialties (Dermatologist and others) during these particular days, for revision and consultation. Every DM case was assigned a file number by the JDC. As mentioned earlier, the data collection period extended from January 1st - April 10th, July 2005. A 150 case of DM patients showing bacterial cutaneous manifestations, out of 4398 of known DM cases, was considered as the study population. For all instances, questionnaires (below) were filled out, and patients were cross- examined by the researcher personally. The questionnaire highlights were: The patient’s serial number, name, sex, age. Patients were categorized as less than 20 years, over 20, over 40, and over 65 years. The marital status was classified as (unmarried, married, divorced, and widow); residence, tribe, occupation, educational background, type of DM (1, 2, 3, and 4). The duration of DM (days, months, or years), associated diseases (hypertension, thyroid swelling, renal, and others), treatment, symptoms (type and duration), signs (distribution and configuration of cutaneous lesions, morphology of individual lesions, lesion color, and palpation of cutaneous lesions), professional diagnosis, confirmatory investigations (14), final diagnosis and comments.Lesions diagnostic criteria that have been followed to define BCMs of DM in patients in this study were:1-Staphylococcus aureus (Furuncles-carbuncles-Styes).A furuncle is an acute, usually necrotic, infection of a hair follicle.A carbuncle is a deep infection of a group of contiguous follicles.2-Pseudomonas aeruginosaFolliculitis and toe web or nail infection.
4. Results
|

|

|

|
5. Discussion
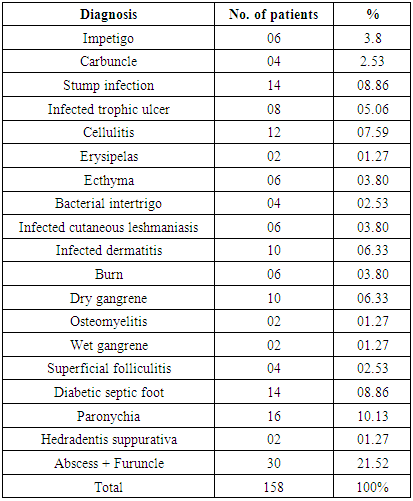
- Table 1: Reveals that 614 patients out of 4398 diabetics who attended JDC, have cutaneous manifestations that are 13.96%; being close to the study done by Bashir [8], which represented 11.24%, still lower than the study of Cohn and Perez [5]; this could be due to the awareness of patients in the western world?Table 2: Shows that the 150 patients with BCM out of the 614 with cutaneous manifestations of the DM subjects, represented 24.42%, a result still close to Bashir’s study which was (26.4%), but higher than the 2 years’ study done in Jordan, 1998-2000 at Princess Haya Hospital-Aqaba, which was 10.3% [2]. It would be due to the highly specialized hospital receiving only severe cases and being elderly patients leading a sedentary life and not exposing themselves to injury. Table 3: Represents the 150 patients with BCM out of the total 4398 which is (3.41%), still close to Bashir’s study of 2001 which was (3.97%).Table 4: Reveals the prevalence of different BCM in this study. Furuncle and abscess forming (19%); the most highly diagnosed, followed by the diabetic septic foot & infected stump, each (8.86%), then cellulitis (7.6%), infected dermatitis (6.33%), gangrene dry and wet (7.6%), paronychia (10.13%), infected ulcers (5%). Peripheral neuropathy and ischemia combined within growing tow nail, leading to foot ulceration afflicting 15% of the diabetics during their life [2].
6. Conclusions
- Of 4398 cases of diabetes mellitus examined for Bacterial cutaneous findings, only 150 diabetic patients (3.6%) showed Bacterial cutaneous lesions.