Noha Ezzat Mohamed1, Youmna Ahmed Elkhazragy2, Naglaa Abo Elfatah Tawfeek3, Wafaa Afifi Hammad2
1Department of Dermatology, Faculty of Medicine, Fayoum University, Fayoum, Egypt
2Department of Dermatology, Faculty of Medicine (for girls), Al-Azhar University, Cairo, Egypt
3Department of Cardiology, Faculty of Medicine (for girls), Al-Azhar University, Cairo, Egypt
Correspondence to: Noha Ezzat Mohamed, Department of Dermatology, Faculty of Medicine, Fayoum University, Fayoum, Egypt.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
Abstract
Backgroundandaimofthestudy:Many reports linked Androgenetic Alopecia(AGA) and ischemicheart disease. We aimed in this study to predict the relation between early androgenic alopecia and ischemic heart disease. Subjectandmethod:This study was conducted on (100) male aged (20-30 years), suffering from early AGA > grade 2 (1) with no history of cardiac disease versus 100 apparently healthy age matched male as a control group with no history of cardiac disease. Measurement of blood Pressure, lipid profile, Resting high-quality 12 lead Electrocardiograms(ECG), Echo-cardiography were done. Results: No significant differences between patients and control group regarding age. The BMI and waist circumference of patient group were significantly higher compared with control. As regard family history: There were significant higher difference regarding positive family history of AGA and C.V.D in cases compared to control. Statistically significant higher level in systolic blood pressure (SBP), cholesterol and triglycerides (TG) in AGA group compared to control group, while no statistically significant differences in diastolic blood pressure(DBP), high and low density lipoprotein level ((HDL) (LDL)) in AGA group. ECG found abnormal finding in 4 AGA patient which was statistically significant. The cases with positive ECG finding undergo ECHO two (2) of them have normal ECHO and the other two (2) cases had mitral valve prolapse, which is considered normal finding in 2-3% of population. As regard family history of AGA; there were statistically significant higher levels of SBP and LDL in 74 cases compared with 26 cases with no family history of AGA. While, there were no statistically significant difference in DBP, TG, TC, HDL and ECG between both groups. As regard risk factors, only SBP and TG were significantly higher according to severity of alopecia but, there were no statistically significant difference regarding DBP, cholesterol, HDL and LDL, as well as ECG findings with increase severity. Smokers had significantly more severe alopecia, SBP, TG, LDL and ECG than non-smoker in patients group. There was significant increase in SBP, TG and HDL in smoker when compared with non-smoker in control group. ConclusionsandRecommendations: AGA could predict ischemic heart disease, all AGA patients should be screened for coronary artery disease.
Keywords:
Ischemic Heart Disease, Androgenetic Alopecia
Cite this paper: Noha Ezzat Mohamed, Youmna Ahmed Elkhazragy, Naglaa Abo Elfatah Tawfeek, Wafaa Afifi Hammad, Early Androgenetic Alopecia as a Predictor of Ischemic Heart Disease, American Journal of Dermatology and Venereology, Vol. 4 No. 2, 2015, pp. 18-25. doi: 10.5923/j.ajdv.20150402.03.
1. Introduction
Androgenetic alopecia (AGA) is a common hair loss disease with genetic predisposition among men and women, and it may commence at any age after puberty. It may significantly affect a variety of psychological and social aspects of one's life and the individual's overall quality of life [2].Hair is lost in a well-defined pattern, beginning above both temples. Over time, the hair line recedes to form a characteristic "M" shape. Hair also thins at the crown, often progressing to partial or complete baldness [3].Alopecia has been associated with an increased risk of coronary heart disease as well as hyperinsulinaemia, insulin resistance, metabolic syndrome, dyslipidaemia, and hypertension [4].The reason for the association between baldness and CHD is unclear. It has been suggested that classical coronary risk factors e.g. (age, hypertension, dyslipidemia and smoking might influence both conditions, so that baldness is a marker of atherosclerosis [5].Chronic inflammation, which is more prevalent in patients with androgenetic alopecia has been shown to play a key role in the presence of insulin resistance, endothelial dysfunction and cardiovascular disease [6].Additionally, androgen involved in the pathogenesis of androgenetic alopecia bind to vascular receptors and favor the increase in blood pressure and hyperaldosteronism, which is an underlying condition in most cases of hypertension that plays a direct role in the development of androgenic alopecia [7].Aim of this study: was to detect the association between early androgenic alopecia and ischemic heart disease.
2. Patients and Methods
Patients: This study was conducted on (100) malepatients aged (20-30ys), selected from dermatology outpatient clinics of AL-Zahraa University Hospital between October 2013 to May 2014 suffering from early androgenic alopecia > grade 2 (1) with no history of cardiac disease. One hundred apparently healthy male in the same age group of the patients were taken as a control group, no history of cardiac disease. We excluded patients with Thyroid disease, Cushing`s disease, liver disease, renal failure, malignancies and autoimmune diseases or patients under (Androgen or anti androgen therapyorhypocholesterolmics, antihypertensive or diuretics drugs, Insulin-sensitizing drugs or insulin treatment and Glucocorticoid treatment) within the previous six months.Methods: Full History taking including family history of AGA and smoking habit, full medical Examination, including ("BMI") and blood pressure measurement, dermatological Examination for diagnosis of androgenetic alopecia (AGA). Measurement of serumlevel of (TC), Triglyceride (TG), (HDL-C), (LDL-C), 12 leads ECGAloca, Japan and Echocardiography (Philps clear view 550, Phlips company USA).
3. Statistical Analysis
The data collected were tabulated and analyzed by SPSS (statistical package for social science) version 19.0 on IBM compatible computer.i. Descriptive statistics: Mean ± standard deviation (SD) and range for numerical data and frequency and percentage of non-numerical data.ii. Analytical statistics: Student t-test: it was used to assess the statistical significance of the difference between two study group means, Chi-Square test: it was used to examine the relationship between two qualitative variables, Correlation analysis: was used to asses strength of association between two quantitative variables. ANOVA test: was used to assess the statistical significance of the difference between more than two study group means and setting of P-value P > 0.05: non-significant. And P ≤ 0.05: significant.
4. Results
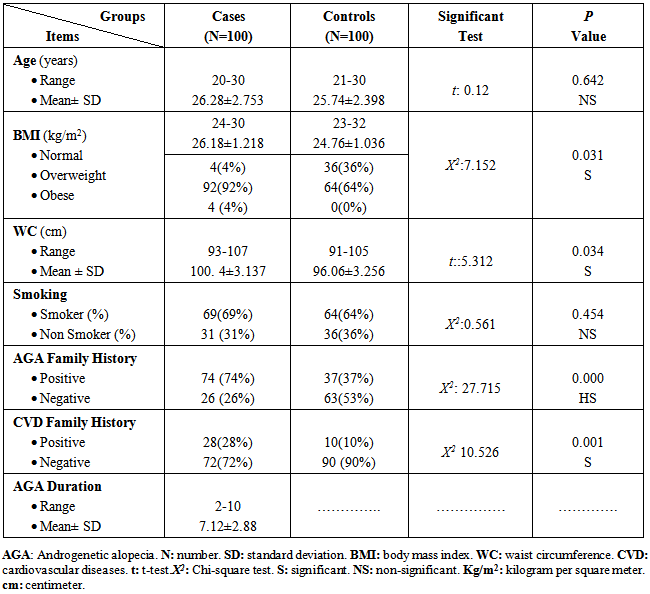
Table (1): No significant differences between patients and control group regarding age. The BMI and waist circumference of patient group were significantly higher compared with control. As regard family history: There were significant higher difference regarding positive family history of AGA and C.V.D in cases compared to control.Table (1). Demographic data of the studied groups
 |
| |
|
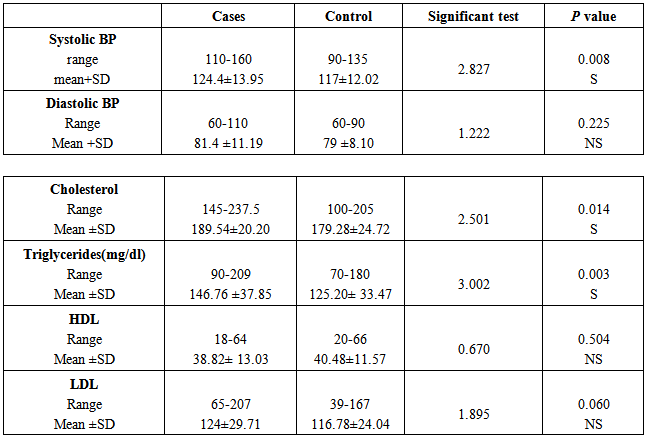
Table (2). Comparison between patients and control group regarding risk factors
 |
| |
|
There was significantly higher level in SBP, TC and TG in AGA group compared to control group (P<.05). While, there was no statistically significant differences in DBP, HDL and LDL in AGA group (P>.05).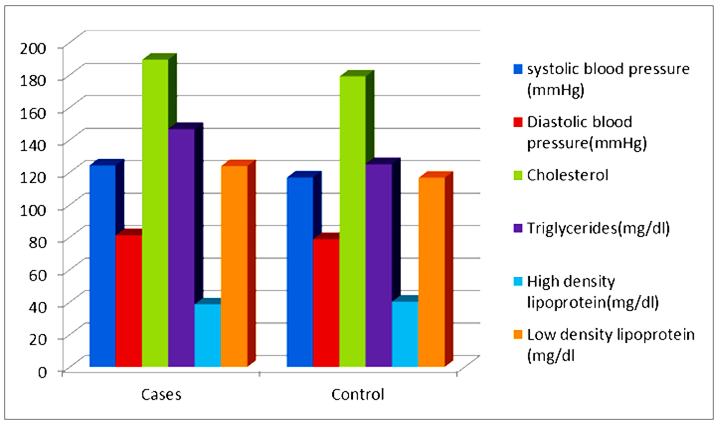 | Figure (1). Blood pressure and Lipid profile presentation in both study groups |
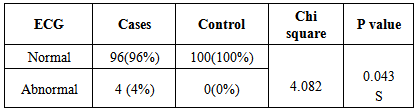
Table (3). ECG Finding in cases and control group
 |
| |
|
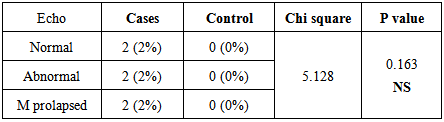
ECG show abnormal finding in 4 AGA patient which was statistically significant high (P<.05).Table (4). Echo finding for ECG positive cases
 |
| |
|
The cases with positive ECG finding undergo ECHO two (2) have normal ECHO and the other two (2) cases had mitral valve prolapse, which is considered normal finding in 2-3% of population(P>.05).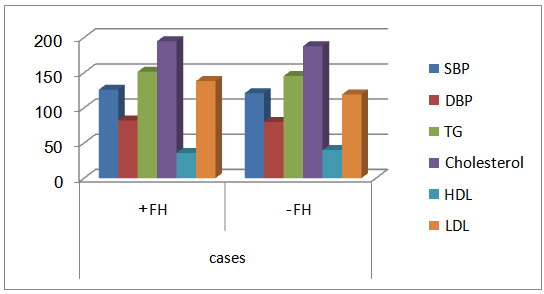 | Figure (2). Comparison of risk factor regarding family history in AGA group |
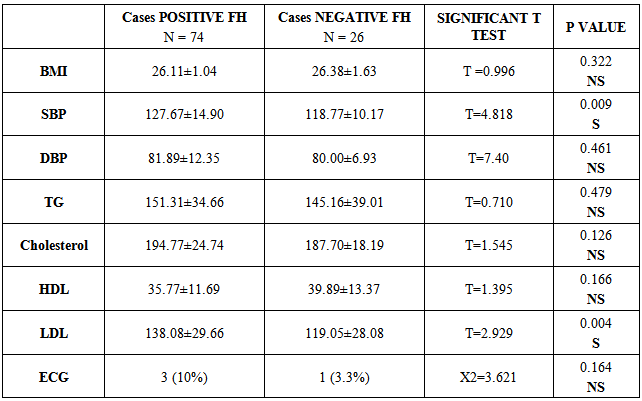
Table (5): showed the family history of AGA group: there were significantly higher level of SBP and LDL in 74 positive cases when compared with 26 cases with no history of AGA. While, there were no statistically significant difference in DBP, TG, TC, HDL and ECG.Table (5). COMparison in patient group with or without positive family history for AGA for risk factors
 |
| |
|
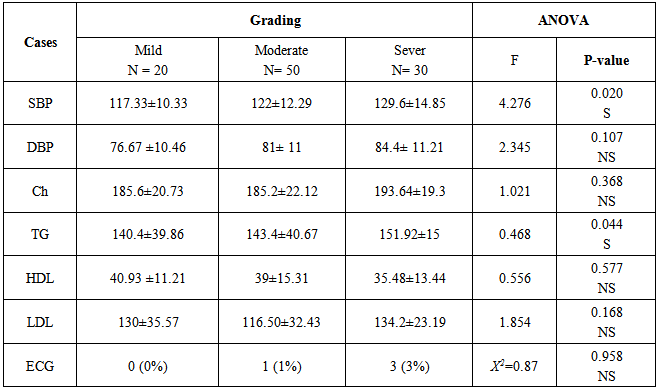
Table (6): As regard risk factors, Only SBP and TG had significantly higher according to severity of alopecia but there were no significant difference for the DBP, cholesterol, HDL and LDL, as well ECG studies with increase severity.Table (6). Comparison between different degrees of AGA of patient group regarding risk factors
 |
| |
|
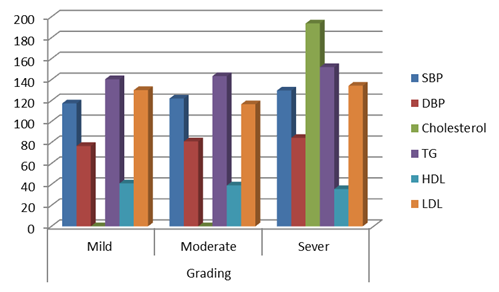 | Figure (3). Comparison of risk factors regarding AGA grading in AGA group |
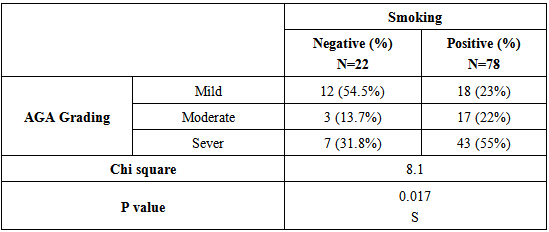
Table (7): Smoker had higher value than non smoker regarding severity of alopecia (p <0.05).Table (7). Effect of smoking on severity of AGA
 |
| |
|
Table (8): As regard to smoking, there were significantly increase of SBP, TG, LDL and ECG ischemic findings in smoker AGA when compared with non smoker AGA. There were significantly increase of SBP, TG and HDL in smoker control when compared with healthy non smoker.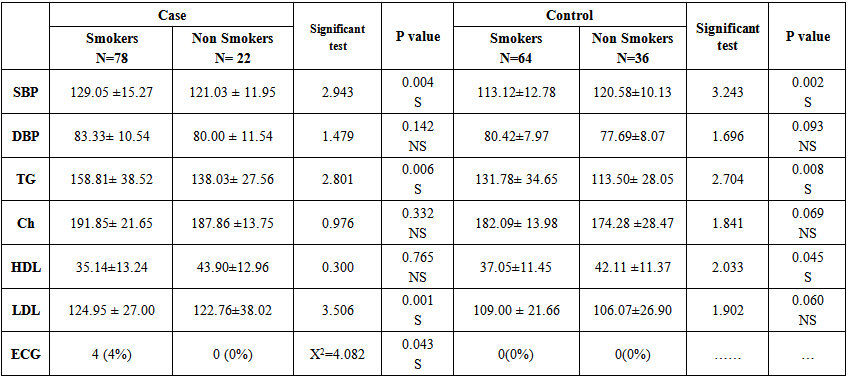 | Table (8). Comparison of risk factor as regard smoking in both studied groups |
5. Discussion
Androgenetic alopecia (AGA) or male pattern baldness (MPB) has been found to be associated with the risk of coronary artery disease (CAD). The well-known riskfactors are family history of CAD, hypertension, increased body mass index (BMI), central obesity, hyperglycemia, and dyslipidemia [8]. The meningeal association between androgeniac alopecia and cardiovascular disease has been well documented, but the causes underlying the association are not clear. It has also been postulated that baldness is linked to CHD by mechanisms such as hyper-insulinaemia, chronic inflammation and increased peripheral sensitivity to androgens [7]. Therefore our study was conducted to evalute the data concerning the traditional cardio vascular risk factor to perdict relation between early onset androgenic alopecia and cardiac disease. Risk of cardiac disease differ according to age and sex, so we have selected our case to be age and sex matched with control. Smoking habit was found in 2/3 of androgenic alopecia patient in present study. However we did not notice difference in smoking habit between cases and control. As smoking itself is major risk factor for cardiovascular disease. The enrollment of smoker is a form of limitation in this study.In the current study, obesity was statistically significant higher among cases compared to control. Both BMI and waist circumference were predominant higher in cases compared with control. This mean that there is a redistribution of abdominal fat associated with androgenic alopecia patient. This is an important cardiovascular risk factor associated with insulin resistance as a part of metabolic syndrome Obesity associated with hyperandrogenism promoting acne vulgarus, hirsutism and androgenetic alopecia [9].The increased prevalence of obesity in androgenic alopecia patient reported by several previous studies by González et al. [10] who did study on 80 young males, aged (18–35) years, with AGA > stage III and 80 weight- and age matched control, Diane et al. [11] who reported that obesity is one of the factors related to causing AGA. And Starka et al. [12] who reported that obesity may be additional factor to AGA for cardiac disease.Controversy was found by (Sherine et al., in which 60 men were enrolled in their study but in small number of patients and control (30 for each) [13]. This observation was supported also by Arias-Santiagos et al. who concluded that the effect of AGA, as a marker of insulin resistance, is not strong enough to identify patients in daily clinical practice, but it could be relevant in epidemiological research. [6].In our study, there was significantly higher level in SBP but not in DBP in AGA compared with control. the severity of systolic hypertension is correlated with severity of alopecia,. This was in agree with Sharma et al. and Sherine et al. [8, 13] who found that patients with AGA show significantly higher Aldosterone level and blood pressure value. Also (Ahouansou et al. offered an explanation for this association; androgen involved in the pathogenesis of AGA binds to vascular receptors and favors the increase in BP [14]. Also the two anti-hypertensive medications have been used to increase hair growth, Minoxidil and Spironolacton.In same line with our study hypertension was reported to be significantly associated with AGA by Arias-Santiagos et al. [7], Matllainen V [15] and Sherine et al. [13]. Also (Ahouansou et Al. found that 82% of patients with hypertension (>140/90 mm Hg) had alopecia compared with 56% of those with normal blood pressure and this association was independent of age [14].However, in 2007, Hirsso et al. did not find a statistically significant difference in SBP and DBP levels in patients younger than 35 years of age compared to control [16].In our series there was statistically significant higher difference in TG and TC in AGA patient compared with control. The pathogenic mechanism of atherosclerosis are quite well known, but the pathogenic link between alopecia and atherosclerosis is not clear. Higher TC and TG levels participate along with other mechanisms initiating atheromatous plaque [7]. Also we found TG level increased with increased severity of alopecia. This was in agree with (Arias-Santiago et al. who found that mean triglyceride values were higher in cases than in control (164.0 mg/dLVs 123.0 mg/dL) [7]. On the same line, Matilainen et al. found similar results in men with alopecia who had undergone revascularization due to heart disease [17]. However, our result did not find statistically significant difference in HDL and LDL between cases and control as their plasma level were strongly associated with physical exercise. The high rate of sedentary lifestyle explain the low HDL-C values and the absence of difference. This was in agree with (Arias-Santiago et al. who found Mean HDL-C values, while somewhat lower in the case of patients with alopecia, but were quite similar [7].On the Contrary, (Sharma et al found that, there was a LDL difference between studied group. LDL thought to be a key determinant of CAD risk and also level of HDL is inversely related to risk. The protective effect of HDL is at least as strong as the atherogenic effect of LDL and is independent of lipids and other riskfactor [8].(Sharrett et al. studied both HDL-C and TG in the general population and confirmed that the association with the presence of athermanousplaque was not very strong; however, both were associated with coronary disease [18].ECG finding in our cases was statistically significant when compared with control. We found 4 patients with abnormal finding But with free echocardiographic findings. This may be explained by ECG can`t predict and it is insufficient method to detect cardio vascular events and to predictathermanous plaque. Also age range of patient was too young to be affected by atherogenic effect of androgen and other risk factor.However, Arias-Santiago et al. found that atheromatous plaque was present in 34% of cases, and 3 of these patients had hemodynamic abnormalities with altered carotid flow. In contrast, only 8.6% of patients in the control group had unilateral atheroma. In addition, carotid intima-media thickness was greater in casesby using Doppler ultrasound and magnetic resonance angiography (7).In our study, there was high statistically significant difference of AGA and CAD family history in cases when compared with control. Similarly Trevisan et al. and Sharma et al. also found that family history of alopecia and cardiac disease were statistically significant higher in cases when compared with control. This indicate avariety of genetic and environmental factors are said to play a role in causing AGA [19-8]. In our patients and according to family history of coronary artery disease, there were statistically significant difference in both systolic blood pressure and LDL in cases with positive family history. While nostatistically significant difference regarding diastolic blood pressure and other risk factor.Our result reported association between smoking and AGA severity, the Smoker had higher severity than non smoker. Also there were statistically significant higher value in both SBP and TG in both smoker cases and control in comparison with non smoker cases and control.The mechanisms by which smoking causes hair loss may be multi-factorial. First, cigarette smoking may be deleterious to the microvasculature of the dermal hair papilla. Second, smoke toxicants may do damage to DNA of the hair follicle. Third, smoking may lead to an imbalance in the follicular protease or anti-protease system [20]. Smoking-induced oxidative substance may lead to the release of proinflammatory cytokines that, in turn, results in follicular microinflammation and fibrosis [21]. Our results were consistent with findings by (Mosley and Lin Hui et al. [21-22] However it is in contrast with (Severi et al. who didn’t find statistically significant association between smoking and AGA [23]. Limitations of our study include small number of patients and control and presence of other factors that linked to ischemic heart disease and androgenetic alopecia that needs further research.
6. Conclusions and Recommendations
There was significantly higher level in SBP, TC and TG in AGA group compared to control group. While, there was no statistically significant differences in DBP, HDL and LDL in AGA group.ECG show abnormal finding in 4 AGA patient which was statistically significant high The cases with positive ECG finding undergo ECHO two (2) have normal ECHO and the other two (2) cases had mitral valve prolapse, which is considered normal finding in 2-3% of population. showed the family history of AGA group: there were significantly higher level of SBP and LDL in 74 positive cases when compared with 26 cases with no history of AGA. While , there were no statistically significant difference in DBP, TG, TC, HDL and ECG.As regard risk factors, Only SBP and TG had significantly higher according to severity of alopecia but there were no significant difference for the DBP, cholesterol, HDL and LDL, as well ECG studies with increase severity. Smoker had higher value than non smoker regarding severity of alopecia. As regard to smoking, there were significantly increase of SBP, TG, LDL and ECG ischemic findings in smoker AGA when compared with non smoker AGA. There were significantly increase of SBP, TG and HDL in smoker control when compared with healthy non smoker. AGA could predict ischemic heart disease, all AGA patients should be screened for coronary artery disease.
References
| [1] | Norwood OT. (1975): Male pattern baldness Classification and incidence. South Med J;68:1359–1365. |
| [2] | Han SH2-Byun JW, Lee WS, Kang H, Kye YC, Kim KH, Kim DW, Kim MB, Kim SJ, Kim HO, Sim WY, Yoon TY, Huh CH, Hwang SS, Ro BI, Choi GS. (2012): Quality of life assessment in male patients with androgenetic alopecia: result of a prospective, multicenter study. Ann Dermatol; 24(3): 311-8. |
| [3] | Amber S. Tully, Justin Schwartzenberger, James Studdiford. (2010): androgenetic alopecia. Journal of Men's Health; 7 (3): 270-277. |
| [4] | Nelson Trieu, Guy D. Eslick (2014): Alopecia and its association with coronary heart disease and cardiovascular risk factors: A meta-analysis International Journal of Cardiology, 176( 3): 687-695. |
| [5] | Wynne F and Khalil RA (2003): Testosterone and coronary vascular tone implication in coronary artery disease. Endocrinal Invest; 26:181-186. |
| [6] | Arias-Santigo S, Gutierrez-Salmeron MT, Castellote- Caballero L and Naranjo-Sintes R (2009): Elevated aldosterone levels in patients with androgenetic alopecia. Br J Dermatol :161:1196-1198. |
| [7] | Arias-Santiago S, Gutierrez-Salmeron MT, Castello-Caballero L, Buendia-Eisman A and Naranjo-Sintes R. (2010): Male androgenic alopecia and cardiovascular risk factors: A case-control study. ActasDermosifiliogr; 101 (3): 248-256. |
| [8] | Sharma L, Dubey A, Gupta P R, Agrawal (2013): Androgeneticalopecia and risk of coronary artery disease. Indian Dermatol Online Journal volume;4:283-287. |
| [9] | Lau k and Hoger PH. (2013): Skin diseases associated with obesity in children. Bund Gesum G j:56(4):539-542. |
| [10] | González-González JG, Mancillas-Adame LG, Fernández- Reyes M, Gómez-Flores M, Lavalle-González FJ, Ocampo-Candiani J, Villarreal-Pérez JZ (2009): Androgenic alopecia and insulin resistance in young men. ClinEndocrinol ; 71:494–499. |
| [11] | Diane R (2010): The basic of balding: Androgenetic alopecia. And insulin ClinEndocrinol :74:258-260. |
| [12] | Starka L, Duskova M, Cermakova I, Vrbiková J, Hill M(2005): Premature androgenic alopecia and insulin resistance. Male equivalent of polycystic ovary syndrome? EndocrRegul. 39(4):127-31. |
| [13] | Sherine H. Abd El-Rahman, Fatma M. El-Esawy (2013): Androgenetic alopecia as an early marker for hypertension Egyptian Journal of Dermatology and Venereology, 33: 63–66. |
| [14] | Ahouansou S, Le Toumelin P, Crickx B, Descamps V (2007): Association ofandrogenetic alopecia & hypertension. Eur J Dermatol ; 17:220–223. |
| [15] | Matllainen V, Hirsso P1, Laakso M, Hiltunen L, Rajala U, Jokelainen J, Keinänen-Kiukaanniemi S(2006): Association of insulin resistance linked diseases and hair loss in elderly men. Finnish population-based study. Cent Eur J Public Health.;14(2):78-81. |
| [16] | Hirsso P, Rajala U, Hiltunen L, J Jokelainen, Keinänen-Kiukaanniemi S, Näyhä S (2007): Obesity and low-grade inflammation among young Finnish men with early-onset alopecia. Dermatology; 214:125–129. |
| [17] | Matilainen VA, Mäkinen PK, Keinänen-Kiukaanniemi SM (2001): Early onset of androgenetic alopecia associated with early severe coronary heart disease: A population-based, case-control study. J Cardiovasc Risk. ; 8:147–151. |
| [18] | Sharrett AR, Sorlie PD, Chambless LE, Folsom AR, Hutchinson RG, Heiss G (2000).: Relative importance of various risk factors for asymptomatic carotid atherosclerosis versus coronary heart disease incidence: The Atherosclerosis Risk in Communities Study. Am J Epidemiol. ;149:843–852. |
| [19] | Trevisan M, Farinaro E, Krogh V, Josssa F, Giumetti D, Fusco G (2000): Baldness and coronary heart disease risk factors. J ClinEpidemiol ;46:1213-1218. |
| [20] | Trüeb RM (2002): Molecular mechanisms of androgenetic alopecia. ExpGerontol; 37 (8-9) 981- 990. |
| [21] | Lin-Hui Su, MD, MSc, Tony, Hsiu-Hsi Chen, DDS, PhD (2007): Association of Androgenetic Alopecia With Smoking and Its Prevalence Among Asian Men: A Community-Based Survey FREE 93, 1834–1840. Arch Dermatol.; 143(11): 1401-1406. |
| [22] | Mosley JGGibbs (1999): AC Premature grey hair and hair loss among smokers: a new opportunity for health education? BMJ; 313 (7072) 16. |
| [23] | Severi G Sinclair R. Hopper JL (2003): Androgenetic alopecia in men aged 40-69 years: prevalence and risk factors. Br. J Dermatol ;149 (6) 1207 - 1221. |
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML