-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Dermatology and Venereology
2014; 3(4): 69-71
doi:10.5923/j.ajdv.20140304.01
A Rare Presentation of Colloid Milium
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLQasim Salim Qasim1, Ali Yaseen Hashim2, Shamil Mahmood Ali3, Inas Sabah2
1Department of Dermatology, College of Medicine, University of Mosul, Iraq
2Department of Pathology, Al Zahrawi Teaching Hospital, Iraq
3Department of Dermatology, Mosul General Hospital, Mosul, Iraq
Correspondence to: Qasim Salim Qasim, Department of Dermatology, College of Medicine, University of Mosul, Iraq.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
Colloid milium is a degenerative change of uncertain etiology, characterized clinically by the development of yellowish, translucent papules or plaques and may rarely be verrucous on light-exposed skin. Pigmented forms of colloid milium associated with hydroquinone use represent ochronosis-like pigmentation. In this case report we present a case of colloid milium in a 55 years old male with verrucous violaceous colloid milium on the dorsum of both hands, face, and ears.
Keywords: Adult, Biopsy, Colloid, Hand, Male, Milium, Skin disease
Cite this paper: Qasim Salim Qasim, Ali Yaseen Hashim, Shamil Mahmood Ali, Inas Sabah, A Rare Presentation of Colloid Milium, American Journal of Dermatology and Venereology, Vol. 3 No. 4, 2014, pp. 69-71. doi: 10.5923/j.ajdv.20140304.01.
1. Introduction
- Adult colloid milium is a rare cutaneous deposition disorder that frequently involves areas of chronic sun exposure, The origin of the colloid deposition in the dermis is not certain, but it is thought to be due to degeneration of elastic fibers in the adult form and due to degeneration of UV‑transformed keratinocytes in the juvenile form [1, 2].Adult colloid milium is characterized by multiple translucent papules on the sun‑exposed areas of the face, neck, dorsum of hands, and back. They feel soft and may release their gelatinous contents when punctured. Lesions often coalesce into plaques, and may rarely be verrucous. Pigmented forms of colloid milium associated with hydroquinone use represent ochronosis-like pigmentation [3]. Although colloid milium may become more severe and more extensive over the years, most cases reach their maximum development within 3 years and then remain unchanged [4].
2. Case Report
- A 55 years old male presented with asymptomatic pigmented verrucous firm papules coalescent to plague on the dorsum of both hands with firm violaceous papules on the forehead, eyelids and ears for 35 years figure (1). He had a chronic and intense sun exposure during adolescent and he claimed to work with petrochemical material but he denied any use of topical hydroquinone or repeated trauma. There is no family history of such skin disease.
 | Figure 1. Pigmented papules involve the dorsum of hands, forehead, periorbital area and ears |
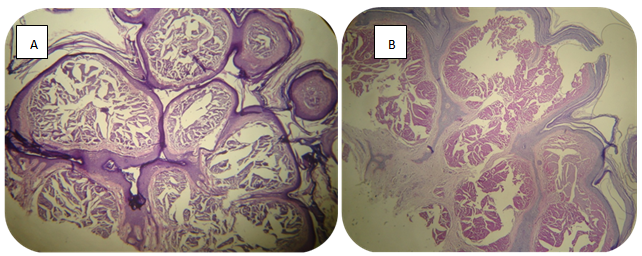 | Figure 2. Nodules of eosinophilic material in the papillary dermis. (A) H&E X4; (B) PAS X4 |
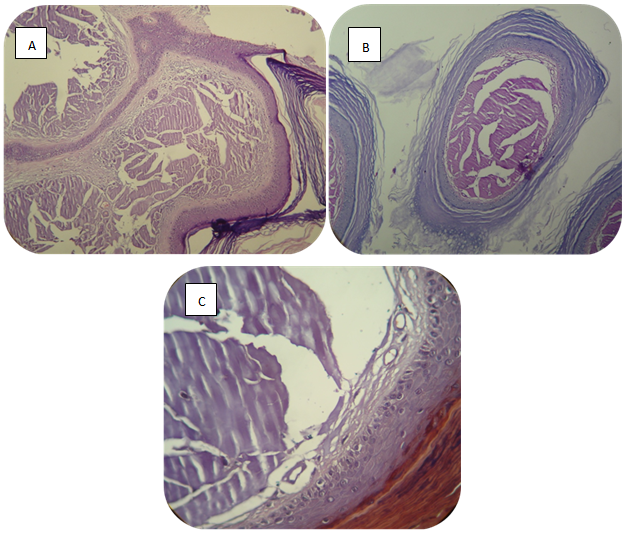 | Figure 3. Cleft and fissures within the nodule of colloid material (A) H&E; (B) PAS X10; (C) congo red X40 |
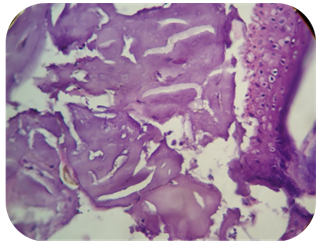 | Figure 4. Fibroblast aligning the fissures and cleft (H&E, X40) |
3. Discussion
- Colloid milium is a degenerative change of uncertain etiology, There are three main forms of colloid milium: adult, juvenile and nodular colloid degeneration type [1, 2]. The main etiology is uncertain although some authors suggest that provoking factors may be due to chronic ultra violate exposure, Analogous changes have been seen when the skin is exposed to certain crude fuels in individuals working in the sun, and phenolic components in the fuels are suspected. [3]Clinically presented as small dermal papules 1–2 mm in diameter, yellowish brown and sometimes translucent, develop slowly and more or less symmetrically in irregular groups in areas exposed to sunlight. They feel soft and may release their gelatinous contents when punctured. Lesions often coalesce into plaques, and may rarely be verrucous. Pigmented forms of colloid milium associated with hydroquinone use represent ochronosis-like pigmentation [3]. In our case it was firm verrucous pigmented papules. The most frequently involved sites are the face, especially around the orbits, the dorsa of the hands, the back and the ears. In adult colloid milium, nodules composed of homogeneous eosinophilic colloid material expanding the papillary dermis & extending into the mid dermis with a grenz zone between nodules & overlying epidermis. Within the nodules, there may be clefts and fissures, and fibroblast are commonly seen aligned along these fissures. The colloid material stain positively with crystal violet, Congo red and thioflavin T stains. In addition, PAS staining is positive but elastic stains are usually negative. In pigmented colloid milium, lightly pigmented islands of colloid material are found in the upper dermis. In this case there is no such pigmented colloid material [5, 6].Treatment modalities are limited and include laser therapy (e.g. longpulsed Er: YAG, fractional photothermolysis), dermabrasion, intense pulsed light, cryotherapy and chemical peels [7-10].
4. Conclusions
- Colloid milium is a rare disease can be presented with variable and extensive skin lesions on the sun exposed area.