-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Dermatology and Venereology
2014; 3(1): 9-12
doi:10.5923/j.ajdv.20140301.03
Direct Electrical Current is A New Therapeutic Option for Vitiligo
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKhalifa E. Sharquie1, Hayder Al-Hamamy2, Adil A. Noaimi1, Mohammed A. Al-Marsomy3, Husam Ali Salman4
1Scientific Council of Dermatology &Venereology-Iraqi and Arab Board for Medical Specializations. Department of Dermatology & Venereology, College of Medicine, University of Baghdad, Baghdad, Iraq
2Chairman of the Scientific Council of Dermatology & Venereology-Iraqi Board for Medical Specializations
3Department of Dermatology & Venereology-Baghdad Teaching Hospital, Baghdad, Iraq
4Head of the Department of Dermatology &Venereology, College of Medicine, University of Baghdad, Baghdad, Iraq
Correspondence to: Husam Ali Salman, Head of the Department of Dermatology &Venereology, College of Medicine, University of Baghdad, Baghdad, Iraq.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
Vitiligo is a common disorder characterized by well circumscribed milky white cutaneous macules devoid of identifiable melanocytes where there is disturbance of the electrical battery of the skin. The aim is to evaluate the effect of direct electrical current in induction of regimentation of vitiliginous patches. It issingle blinded, controlled therapeutic study. The number and size of involved patches were measured and direct electrical current was used to treat a single patch in each patient while the other patches were left as control. The Baghdadin device was used to give direct electrical current between 5-10 milliamperes and a voltage less than 40 volts. Treatment sessions of 10 minutes duration were given at weekly intervals for 5 months. Patients were evaluated monthly according to the grade of response to treatment till the end of the study and to report any local or systemic side effects. Twenty-two patients completed the study. On follow up, there was an obvious repigmentation and reduction in the size of patches and this reduction were statistically significant. In conclusion directelectrical current is an effective and safe method of treatment in patients with vitiligo.
Keywords: Directelectrical current, Vitiligo, Therapy
Cite this paper: Khalifa E. Sharquie, Hayder Al-Hamamy, Adil A. Noaimi, Mohammed A. Al-Marsomy, Husam Ali Salman, Direct Electrical Current is A New Therapeutic Option for Vitiligo, American Journal of Dermatology and Venereology, Vol. 3 No. 1, 2014, pp. 9-12. doi: 10.5923/j.ajdv.20140301.03.
1. Introduction
- Vitiligo is an acquired pigmentary disorder characterized by depigmented macules and patches secondary to the loss of functional melanocytes [1-4]. In addition inflammatory immune reaction could be usually seen in the epidermis and dermis [5].There are a variety of treatments available, including topical and systemic therapies [6]. There is an electrical battery is present in the epidermis [7] and is disturbed in many skin diseases like psoriasis and vitiligo [8-10]. Direct electrical current delivered by Baghdadin device. It has been used as effective therapy for cutaneous leishmaniasis [11] and alopecia areata. This encouraged us to apply an external direct electrical current to stimulate the regeneration of melanocytes in patients with vitiligo.
2. Patients and Methods
- The study was conducted at the Department of Dermatology and Venereology, Baghdad Teaching Hospital during January 2002 to April 2003. Thirty-five patients with vitiligo were recruited.Patients with localized vitiligo were selected who had either single or multiple small patches, excluding active lesions and vitiliginous areas on acral parts of the body.The duration of lesions ranged between two months to three years with a mean + SD of 21.2 + 9.1 months.All patients were thoroughly assessed regarding duration, activity of the disease and other autoimmune disease. Also number, size and site of the patches were assessed.From each patient, formal consent was taken before the start the therapy, after full explanation about the goal and nature of the present study, the nature of the disease, course its complications, the method of treatment, duration, cost, side effects of therapy and duration of follow up, prognosis and the need for pre and post treatment photographs. Also, the ethical approval was carried out by the Scientific Council of Dermatology & Venereology-Iraqi Board for Medical Specializations.All patients were photographed by a digital camera as a baseline and then every two months, in the same place with fixed illumination and distance by using a digital camera (Sony: Cyber shoot with resolution 7 mega pixels). From each patient one patch was treated with direct electrical current and other patches were left as control. All the treated and control patches were site matched.The Baghdadin device [11] was used to give a direct electrical current as treatment for patches of vitiligo using suitable voltage and amperage.Baghdadin device consists of the following parts:-1. A Transformer and a bridge-rectifier to change alternating current of 220 V into direct current.2. A voltmeter to display the out-put voltage.3. A potential divider.4. An ammeter to display the current intensity which passes through the lesion.5. Two changeable electrodes made of stainless steel and covered by a piece of gauze soaked in physiologic saline.One electrode (The active) was applied to the lesion, while the other (the dispersive) was applied to a healthy skin away from the lesion. The dimensions of the active electrode depend on the size of the lesion to be treated, which should be completely covered by the gauze. The dispersive electrode must be larger in size than the active one in order to disperse the current. The potential divider was used to decrease the current intensity to zero at the start and at the end of the treatment session. The current intensity ranged between 5-10 milliamperes depending on the site and size of the lesion. The voltage was kept under 40 v in all treatment, smaller lesions required lower current intensities than larger lesions.The treatment protocol consisted of ten-minute sessions given at weekly intervals for 5 months. Patients were seen monthly till the end of the study.The treatment was conducted with the patient in the sitting position. Before starting the treatment, the area should be washed with physiologic saline. The current was then raised from zero, gradually over one minute to the desired level 10 milliampere. It was kept at this level for ten minutes and then gradually reduced to zero before the device was switched off. The lesion was inspected after the end of the treatment session. Few points must be considered before and during the treatment:1. The patch must be completely covered by the active electrode to ensure the passage of current into the whole lesion.2. There must be not contact between the skin of the patient and the metal electrode, otherwise a burn may result. Contact must be through wet gauze. This applies to both the active and the dispersive electrodes.3. The gauze must be completely soaked with physiologic saline. Dry gauze is a poor conductor of electricity.4. The treatment should be started and ended with the current reduced to zero. Raising and decreasing the current intensity should be very gradual, as sharp changes may be associated with pain and muscle spasm.Twenty-two patches were treated and 13 patches left as a control. Surface area was measured before treatment and monthly thereafter.The outline of the treated patch was drawn on transparent paper and the surface area was measured with a graph paper, by counting the number of 2cm.
3. Results
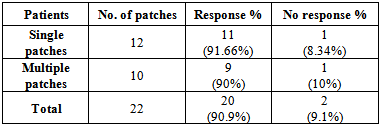
- Twenty-two patients completed the study. Fourteen (63.6%) were females and eight (36.4%) were males; their ages ranged between 13-43 years with a mean ± SD of 19.2 ± 10.1 years. Site of lesions was illustrated in table -1. The legs were the most frequently treated areas. The surface area of vitiligo patches ranges from 0.35 2cm to 22.5 2cm with a mean ± SD of 6.94 ± 3.8 2cm.
|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||
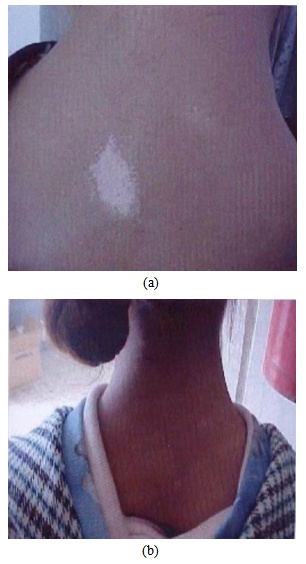 | Figure 1. (a) A patch of vitiligo on the back of the neck of a 16 years old female. (B) After 5 months of treatment with direct electrical current |
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
4. Discussion
- The skin is considered as a battery with the negative potential in the stratum corneum [13]. There are many skin diseases that might alter this battery through changing the surface of the skin and changing the electric potential like psoriasis and vitiligo [10, 14]. Also electric field has profound effects on living cells and tissues [10].Vitiligo is a common disfiguring disorder and many modalities of therapy have been used for its treatment like topical steroids [15]. UVB photo-therapy [16], tincture iodine 5% [17] and direct melanocytes transplant from normal donor skin into vitiliginous recipient skin [18].Direct electrical current had been used as new mode of effective therapy for patients with cutaneous leishmaniasis [11] and alopecia areata.These observations encouraged us to conduct the present work to evaluate the effect of direct current on vitiliginous areas.The response to treatment started in the first month of therapy and this increased gradually over months and the mean of reduction in the vitiliginous areas was 46.6% after 5 months of therapy The duration of therapy is comparable to other treatment modalities with absent side effects such as burning or intense erythema is usually seen with other lines of topical therapy.Also, it is cost-effective therapy when compared with other therapeutic agents like UVB, psoralins, topical 5% tincture iodine, excimer laser and narrow band UVB. This new therapy could be used for stable patches of vitiligo. The mode of action of direct current is not well understood but it might be related to its immunomodulatory effect, its effects on the inflammatory cells movement and on the expression of cellular receptors [10].
5. Conclusions
- Direct electrical current is an effective method to induce melanogenesis in patients with vitiligo.
References
| [1] | Sarquie KE. The Histology and Immunopathology of vitiligo Ph.D. Thesis University of Sheffield, England, 1981. |
| [2] | Sharquie KE. Stages of depigmentation in Vitiligo. Iraqi Medical J 1988; 36: 47-50. |
| [3] | Sharquie KE. Vitiligo Postgraduate Doctor Middle East 1990; B.3:138-42. |
| [4] | Sharquie KE. Vitiligo in Iraq. Iraqi Medical J 1987; 35:2; 31-2. |
| [5] | Sharquie, K.E.; Mehenma, S.H.; Naji, A.A.: Inflammatory changes in vitiligo (stage I and stage II Depigmentation) Animals de dermatologic et al. venereologic: HORS SERIEL (Chirel); 2002: 129 P 277. |
| [6] | Bacigalupi RM, Postolova A, Davis RS. Evidence-based, non-surgical treatments for vitiligo: a review. Am J Clin Dermatol. 2012 Aug 1; 13(4):217-37. |
| [7] | Whitton ME, Pinart M, Batchelor J, Lushey C, Leonardi-Bee J, González U. Interventions for vitiligo. Cochrane Database Syst Rev. 2010 Jan 20; (1):CD003263. |
| [8] | Barker AT, Jaffe LF, Vanables JW. The glabrous epidermis of cavies contains a powerful battery. Am J Physiol (1982): 242 (Regulatory Integrative Comp Physiol 11): R358-R366. |
| [9] | Sharquie KE, Al-Assaf F. Sweating in vitiligo in relation to electrical skin resistance. J Fac Med Baghdad 1985; 27; 4: 49-53. |
| [10] | Al-Hamamy HR. Electrical activity of the skin in health and disease; PhD thesis, University of Baghdad, 1996. |
| [11] | Sharquie KE, Al-Hamamy H, El- Yassin DJ. Treatment of cutaneous leishmaniasis by direct current therapy. The Baghdadian device. J Dermato (Japan) 1998; 25:234-37. |
| [12] | Sami Sasi Younis, Efficacy of PUVA therapy vs NB-UVB therapy. ARC Dermatol. May 2007; 143: 578-584. |
| [13] | Assimacopoulos D. Low intensity negative electr cal current in the treatment of ulcers of the leg due to chronic venous insufficiency. Am J Surg 1969; 115: 683- 687. |
| [14] | Al-Hamamy HR, Sharquie KE, El-Yassin D. Electrical potential recorded from the skin of patients with psoriasis as compared to healthy individuals. J Fac Med 2000; 42: 469-73. |
| [15] | Crimes P, Vitiligo an over view of therapeutic approaches. Dermatol clin 1993; 11: 325-38 |