K S Dhillon , Kshitij Saxena , Gaurav Sarin , Mohd Sadiq Umar
Department of Dermatology, ERA’S Lucknow Medical College and Hospital[ELMC & H] & Research Centre, Lucknow, Uttar Pradesh, India
Correspondence to: Kshitij Saxena , Department of Dermatology, ERA’S Lucknow Medical College and Hospital[ELMC & H] & Research Centre, Lucknow, Uttar Pradesh, India.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Abstract
Melasma, is a commonly acquired symmetric hypermelanosis, characterized by irregular light to dark brown macules, involving the cheeks, forehead, upper lip, nose, and chin. Various combinations of topical medications are being used to treat melasma but chemical peels like Glycolic Acid (GA) and Tri-Chloroacetic Acid (TCA) are proving to be safer, faster and more result oriented options. We compared the efficacy of GA peel, TCA Peel and Placebo in treating Melasma. Initially, priming of facial skin was done by Modified Kligman’s regimen for 2 weeks. Chemo-exfoliation was done every 14 days for 4 sittings and patient was advised daily sunscreen application. Two groups were made, one group of 20 patients receiving GA (50-70%) on right side of face and TCA (10-20%) on the left side (same patient). Second group was of 12 patients receiving Normal Saline (Placebo). Response was assessed by the following criteria - photographs, subjective and clinical improvement. Overall response, evaluated by MASI scoring after 10 weeks, was 64.67 % - GA, 38.09 % - TCA, 33.33 % - Placebo (only sunscreen). Individual response to various chemicals was 61.90 % - GA, 35.0 % - TCA, 26.82 % - Placebo. GA showed better results, tolerability & had an advantage of facial rejuvenation over TCA. Minimal improvement was seen in placebo group.
Keywords:
Melasma, Trichloroacetic Acid, Glycolic Acid, Chemo-exfoliation
Cite this paper:
K S Dhillon , Kshitij Saxena , Gaurav Sarin , Mohd Sadiq Umar , "Comparison of Therapeutic Efficacy of Chemo-exfoliation with Tri-Chloroacetic Acid, Glycolic Acid & Placebo in Melasma", American Journal of Dermatology and Venereology, Vol. 1 No. 2, 2012, pp. 24-29. doi: 10.5923/j.ajdv.20120102.02.
1. Introduction
Melasma is a common, acquired, symmetric hypermelanosis, characterized by irregular light to dark brown macules and patches commonly involving the cheeks, forehead, upper lip, nose, and chin[1]. It is the most common pigmentary disorder among Indians[2]. One of the common aesthetically displeasing entity, it continues to be a difficult problem to treat[3]. Various combinations of topical medications like hydroquinone, tretinoin and topical steroids are used for melasma but chemical peeling provides more rapid response than topical therapy[4]. Various chemical agents have been used and each has its own unique features and produces peeling at different depths[5],[6].Glycolic acid (GA) and Tri-Chloroacetic acid (TCA) have been used alone and also in combination to treat melasma[7],[8]. Although both TCA and GA are being used in various centers in India, there have been very few studies comparing these two agents with placebo in pigmented patients (Fitzpatrick skin type III to V) with melasma, using both subjective and objective methods of evaluation like, Melasma Area Severity Index (MASI). This prompted us to compare the efficacy and side effects of these two easily available agents, TCA and GA with each other and placebo.
2. Aim
Comparison in efficacy of Glycolic Acid &Tri-Chloroacetic Acid peels with Placebo in Melasma.
3. Objectives of the Study
1. To assess the therapeutic response toChemo-exfoliation with TCA & Glycolic Acid.2. To compare the response with TCA, Glycolic acid & Placebo.
4. Material and Methods
4.1. Work Plan
1. Study Design was Prospective study of duration for 4 months.2. Inclusion Criteria – All the patients of Melasma attending the Skin OPD except the Exclusion Criteria.3. Exclusion Criteria – Patients with a history of Herpes, taking Oral Contraceptive Pills,Isotretinoin, Pregnancy, Lactation, Keloids orHypertrophic Scars Tendency, Concomitant Systemic or Skin disease, those with Un-realistic expectations and non-consenting patients were excluded from the study.4. Methods of Selection – Randomization.5. Interventions – Priming with modified Kligman’s formula & regular use of Sunscreen (SPF 30). Peeling with Glycolic Acid, TCA or Placebo was done.6. The study was carried out on 32 patients with epidermal and mixed melasma, visiting the skin outpatient department of our hospital (Wood’s Lamp Examination). 7. These 32 patients were randomized into two groups one of 20 patients for GA and TCA, other of 12 patients of Placebo. 8. A detailed history was taken and clinical examination was performed under natural light to select cases of epidermal and mixed melasma.9. Color digital photographs were taken of all patients under standard conditions in natural light.10. Priming was done for 2 weeks where patients were advised to apply topical sunscreen daily[Sun Protective Factor-30 (SPF-30)] during day time and Modified Kligman’s regimen (Hydoroquinone 2% + Tretinoin 0.025% + Mometasone Furoate 1%) at night. Modified Klingman’s formula was applied at night time less 2 days prior of starting study.11. Prior to application, a written informed consent was obtained. 12. A retro-auricular test peel was performed and left for 15-20 minutes to find any hypersensitivity to the ingredients of peeling agent in GA and TCA.13. Patients were divided into two groups, one of 20 receiving Glycolic Acid (GA) 50-70% on one side of face & Tri-Chloroacetic Acid (TCA) 10-20% on the other side; we did so to know the comparative effect of both peels on the same patient & in the second group of 12 Normal Saline was used as placebo. 14. Applications were done every 14 days till four sittings. 15. Response was assessed by three main criterion :15.1. Clinical photographs of consenting patients were taken.15.2. Subjective improvement as experienced by patient.15.3. Clinical response as assessed by physician at every sitting by calculating MASI (Melasma Area Severity Index).16. Before application of the peeling agent, patients were advised to wash face with soap and water. After patting the face dry, cleansing was done with spirit and then acetone soaked sponges to remove all cutaneous oils & debris. 17. In Glycolic acid group, 50% of GA was applied on right side of face of patient till erythema or maximum of 5 minutes and Tri-Chloroacetic acid 10% TCA was applied on the left side of face of patient till frosting or maximum of 5 minutes on the first 2 sittings. 18. In the subsequent two sittings, the concentration was increased to 70% of Glycolic acid and 20% of TCA, respectively. 19. Neutralization was done with cold water. 20. In the Placebo group, Normal Saline was applied all over the face.21. Post peel topical sunscreen of SPF 30, was advised in all the groups.
5. Results
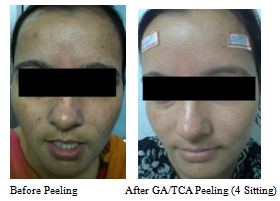
There were 32 patients included in the study. There were 28 females and 04 males with age ranging between 18 and 45 years (mean age of 31years). Duration of Melasma ranged between 1 to 7 years. There were significant precipitating factors observed in relation to occurrence of melasma like relation to pregnancy, intake of oral contraceptive pills, sunlight exposure. Most cases were of epidermal type (78%) and one-fourth of the cases were of mixed type of melasma (22%). The most common pattern was centro-facial pattern. | Figure 1. Group 1 (GA / TCA application) |
 | Figure 1. Patient A (Group1 GA / TCA application) |
 | Figure 2. Patient B (Group 1GA / TCA application) |
Patients were divided into two groups: one group of 20 patients receiving Glycolic Acid (GA) 50-60% on right side of face & Tri-Chloroacetic acid (TCA) 10-15% on the left side of face. In the second group of 12 patients, Normal Saline was used as placebo. On the Glycolic acid right side of face, pre-priming mean MASI was 4.53 with min MASI 0.9 & max MASI 09. After priming the mean MASI came down to 4.2 & after four sittings of peeling mean MASI further came down to 1.6. In total, 61.90 % improvement was seen after 4 sittings of glycolic acid, overall was 64.67 % improvement. In the TCA (left side of face) pre-priming mean MASI was 4.2 with min MASI of 0.9 & max MASI of 09. After priming, the mean MASI came down to 4.0 & after four sittings of peeling mean MASI further came down to 2.6. A total 35.0 % was seen after 4 sittings of TCA, overall was 38.09 % improvement (Fig 1, 2, 4, 5 & Tab 1).In placebo group (whole face) pre-priming mean MASI was 4.5 with min MASI of 0.9 & max MASI of 09. After priming the mean MASI came down to 4.1 & after four sittings of placebo mean MASI further came down to 3.0. A total 26.82 % was seen after 4 sittings in placebo group, overall was 33.33 % improvement (Fig 3-5 & Tab 1, 2). | Figure 3. Patient C (Group 2 Placebo application) |
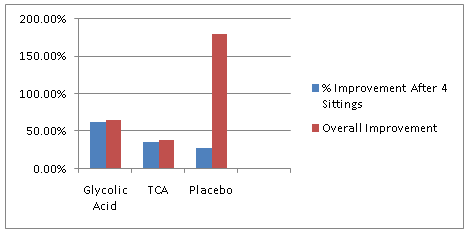 | Figure 4. Showing comparison (in %) of improvement of GA/TCA peel group & Placebo group |
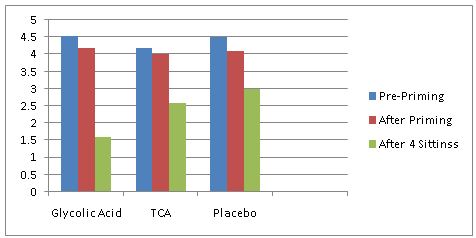 | Figure 5. Showing comparison in MASI Score reduction from start of GA/TCA peel in group one & Placebo in group two till last |
| Table 1. Comparison in reference to Melasma Area Severity Index between Glycolic Acid/TCA peel group & Normal Saline group |
| | | Pre-PrimingMASI (Score) | After PrimingMASI (Score) | After 4 SittingMASI (Score) | Percentage of Improvement in MASI After 4 Sittings | Over All ImprovementIn MASI | | Glycolic Acid | 4.53 | 4.2 | 1.6 | 61.90 % | 64.67 % | | TCA | 4.2 | 4.0 | 2.6 | 35.0 % | 38.09 % | | Placebo | 4.5 | 4.1 | 3.0 | 26.82 % | 33.33 % |
|
|
Post-inflammatory hyper-pigmentation (PIH) was seen in 02 patients, post peel cracking was common due to TCA but 03 patients left because of it. Post peel burning was also common in both GA & TCA peel, but 02 patients left due to the same. 03 patients did not turned up on regular follow-up.Subjective response, as graded by the patient, showed good or very good response in 75% in GA group and 30% in TCA group & 20% in Placebo group. No relation of treatment response to age or duration of melasma could be established in this study (Fig. 6).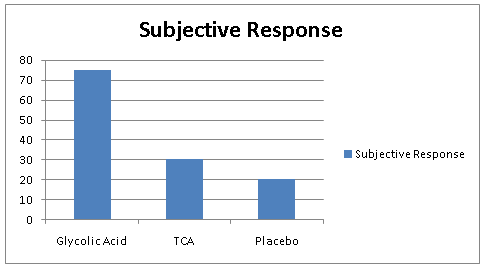 | Figure 6. Showing comparison of subjective response improvement in GA/TCA peel group & Placebo group |
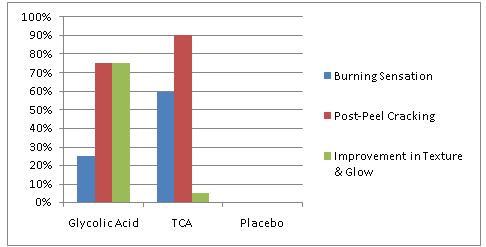 | Figure 7. Showing comparison(in%) of side effects of GA/TCA peel group one & Placebo group two |
There was mild burning sensation in 95% of patients in GA group compared to moderate to severe burning in 75% of patients in the TCA group. Post-peel cracking was reported in 90% of cases in TCA group but in none of the patients in the GA group. There was significant improvement in the texture and glow of skin appreciated by 75% of the patients in GA group, which was not appreciated in TCA group. Placebo group had no complains (Tab 2, Fig 7).So this study demonstrated that Glycolic acid peel is a better peeling agent with lesser side effects as compared to TCA peel in treatment of melasma. However, Placebo group shown only 33.33% of benefit in management of melasma.| Table 2. Showing comparison of side effects & % of improvement in GA/TCA peel group & Placebo group |
| | | Burning Sensation | Post Peel Cracking | Improvement in Texture & Glow | | Glycolic Acid | Mild | 75 % of Patients | 75 % of Patients | | TCA | Moderate to Severe | 90 % of Patients | Not Appreciable | | Placebo | Nil | Nil | Nil |
|
|
6. Discussion
Melasma is more common in women of child-bearing age[9], although men also suffer from this condition and account for 10% of the cases[10]. Melasma affects all races, but is observed more frequently among individuals with skin type IV-VI, especially in women of Hispanic, Caribbean and Asian origin, who live in areas of intense ultraviolet radiation[3]. There are three clinical patterns - centrofacial, malar, and mandibular - depending upon the area of localization[1]. Histologically, melasma is divided into three types: epidermal, dermal, and mixed[11]. Wood's light causes intensification of pigmentation in epidermal-type melasma, but does not enhance the pigmentation in the dermal type. But this distinction may not be useful in pigmented races. A combination of epidermal and dermal macules is recognized as the mixed type[12].Chemical peeling aims at production of controlled chemical burns of epidermis and dermis, resulting in exhalation and subsequent resurfacing of the epidermis and remodeling of collagen and elastic fibers with deposition of glycosaminoglycans in dermis.Application of TCA to the skin causes precipitation of proteins and coagulative necrosis of cells in epidermis. In higher concentration, it causes necrosis of collagen in the papillary to upper reticular dermis. Over several days, the necrotic layers sloughs and the skin re-epithelizes from the germinative segments of hair follicles[3].The benefits of Alpha Hydroxy Acid (AHAs) have long been recognized[13]. Cleopatra, for example, applied sour milk (contains lactic acid) to her face, while Polynesian women found sugarcane juice (contains GA) to provide them with similar benefits. AHAs decrease corneocyte cohesion leading to sloughing of dead cells and stimulation of new cell growth in the basal cell layer. In higher concentrations, they cause epidermolysis. Products with a small molecular size per volume are more active and penetrate the skin more deeply. GA has the smallest molecular structure, followed by Lactic, Pyruvic, Malic, Tartaric and Citric Acids. The bioavailability of AHAs increases as the pH decreases (desirable pH 2.8-4.8), and they are the only peels that are time dependent and can be neutralized easily[15].In our study, the average age of patients of melasma was 31yrs of age, but other studies reported from India, like by Kimbrough-Green et al.[16] reported a much higher age of onset (44 years) of Black patients. The types of melasma in our patients is similar to those studied by Kimbrough-Green et al.[11] in Black women , Griffiths et al.[17] in Caucasian women and Sanchez et al.[6] which all state centrofacial pattern to be the most common.Post-inflammatory hyperpigmentation has been reported to be the most common side effect with GA facial peels[18] but in our study the frequency of post inflammatory hyperpigmentation was much lower as compared to that of other studies[2]. This may have been due to the graded concentration method of acids used and strict adherence to photoprotection. The fewer side effects that occurred like mild erythema and burning sensation were mostly well tolerable and no intervention was done for that. No patient developed vesiculation or keloids after peeling as was reported in other studies. Regular use of sunscreens helped in maintaining the result of the peels on follow up. Post-peel cracking occurred after TCA peel and not with GA makes it beneficial for patients to continue outdoor activities and office work in GA group[19]. In TCA group, many patients took leave from their work to avoid facing their colleagues but in GA group patients were not embarrassed in any way and the glow due to facial rejuvenation made them look appreciably younger.Overall 64.67% improvement was seen in glycolic group, 38.09 % was seen in TCA group and placebo has shown only 33.33% of benefit in management of melasma. In conclusion, GA peel is a better and safer option than a TCA peel. The TCA peel is associated with local reactions. The high cost of GA compensates by the less number of leave period patient may require during the procedure. Sun protection should continue irrespective of the topical therapeutic modalities being used to treat melasma.
References
| [1] | Lapeere H, Borne B, Schepper S, Verhaeghe E, Ongenae K, Geel NV. Hypomelanosis and hypermelanosis. In: Wolff K, Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, editors. Dermatology in General Medicine, 7 th ed. New York: McGraw-Hill; 2008. P. 622-40. |
| [2] | Pasricha JS, Khaitan BK, Dash S. Pigmentary disorders in India. Dermatol Clin 2007;25:343-522. |
| [3] | Grimes PE. Melasma. Arch Dermatol 1995; 131:1453-1457. |
| [4] | Sarkar R, Kaur C, Bhalla M, Kanwar AJ. The combination of glycolic acid peels with a topical regimen in the treatment of melasma in Dark-skinned patients: a comparative study. Dermatol Surg 2002;28:828-32. |
| [5] | Brody HJ. The art of chemical peeling. 3 Dermatol Sung Oncol 1989; 15:918. |
| [6] | Rubin MG. What are skin peels. Manual of chemical peels superficial and medium depth winters SR, James M, Caputo GR eds) Ist edn, Philadelphia. JB Lippencot Co. 1995:17-25. |
| [7] | Garcia A, Fulton JE Jr. The combination of glycolic acid and hydroquinone or kojic acid for the treatment of melasma and related conditions. Dermatol Surg 1996;22:443-447. |
| [8] | Lawrence N, Cox SE, Brody HJ. Teatment of melasma with Jessner's solution versus glycolic acid: a comparison of clinical efficacy and evaluation of the predictive ability of Wood's light examination. J Am ACad Dermatol 1997; 36:589-593. |
| [9] | Karen JK, Pomeranz MK. Skin changes and diseases in pregnancy. In: Wolff K, Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, editors. Dermatology in General Medicine, 7th ed. New York: McGraw-Hill; 2008. P. 955-62. |
| [10] | Vazquez M, Maldonado H, Benaman C, Sanchez JL. Melasma in men: A clinical and histologic study. Int J Dermatol 1988;27:25-7. |
| [11] | Sanchez NP, Pathak MA, Sato S, Fitzpatrick TB, Sanchez JL, Mihm MC Jr. A clinical light microscopic, ultrastructural and immunofluorescence study. J Am Acad Dermatol 1981;4:698710. |
| [12] | Gilchrest BA, Fitzpatrick TB, Anderson RR, Parrish JA. Localization of melanin pigmentation in the skin with Wood's lamp. Br J Dermatol 1977;96:245-8. |
| [13] | Nguyen TH, Rooney JA. Trichloroacetic acid peels. Dermatol Ther 2000;13:173-82. |
| [14] | Javaheri SM, Handa S, Kaur I, Kumar B. Safety and efficacy of glycolic acid facial peel in Indian women with melasma. Int J Dermatol 2001;40:354 |
| [15] | Salvin JW. Considerations in alpha hydroxyacid peels. Clin Plast Surg 1998;25:45-52. |
| [16] | Kimbrough-Green CK, Griffiths CE, Finkel LJ, Hamilton TA, Bulengo-Ransby SM, Ellis CN, et al. Topical retinoic acid (tretinoin) for melasma in black patients. Arch Dermatol 1994;130:727-33. |
| [17] | Griffiths CE, Finkel LJ, Ditre CM, Hamilton TA, Ellis CN, Voorhees JJ. Topical tretinoin (retinoic acid) improves melasma. A vehicle- controlled, clinical trial. Br J Dermatol 1993;129:415-21. |
| [18] | Moy LS. Superficial chemical peels with alpha-hydroxy acid. In: Robinson JK, Andt KA, Wintroub BU, editors. Atlas of Cutaneous Surgery, 1 st ed. Philadelphia: WB Saunders; 1995. P. 345-51. |
| [19] | Ditre CM. Glycolic acid peels. Dermatol Ther 2000;13:165-72. |
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-Text HTML
Full-Text HTML