-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Computational and Applied Mathematics
p-ISSN: 2165-8935 e-ISSN: 2165-8943
2019; 9(2): 43-49
doi:10.5923/j.ajcam.20190902.03

Statistical Analysis of Trends of Malaria Diagnosis and Patient Demographics: A Multivariate Study of Clinic Data in Ghana
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLBosson-Amedenu Senyefia1, Vivian Nimoh1, Osei-Asibey Eunice2
1Department of Mathematics and ICT, Holy Child College of Education, Western Region, Ghana
2Department of Mathematics and ICT, Ada College of Education, Ada Foah, Greater Accra Region, Ghana
Correspondence to: Bosson-Amedenu Senyefia, Department of Mathematics and ICT, Holy Child College of Education, Western Region, Ghana.
| Email: |  |
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

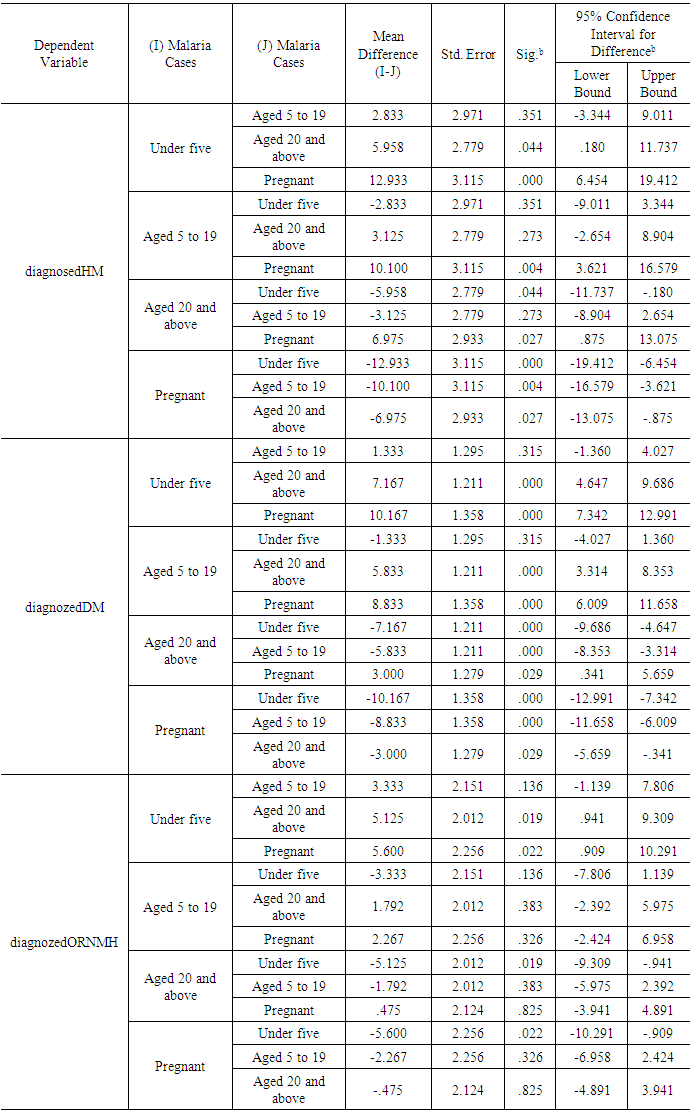
Multivariate analysis was applied to hospital data in this study. The underlying assumptions of MANOVA were verified with the data and were satisfied. The results from the post hoc test showed a positive and significant mean difference between children below the age of five years and patients between the ages of 5 and 19 years (MD=3.333, P<0.05). This means children below the age of five are more vulnerable and prone to hospitalization resulting from malaria infection than patients between the ages of 5 and 19 years. Similarly, there was a positive and significant mean difference (MD=12.933, P<0.05) between children below the age five years and pregnant women. This finding means that once again, children below the age of five are more vulnerable and prone to hospitalization resulting from malaria infection than pregnant women. Also, there was a positive mean difference between patients who were at least 20 years old and pregnant women (MD=10.100, P<0.05) when compared on the basis of hospitalization resulting from malaria infection. This indicated that patients who are at least 20 years old are hospitalized (due to malaria infection) more than pregnant women. With reference to the category of patients who were treated and discharged as a result of malaria infection, there was a positive and significant mean difference between patients who were between the ages of 5 and 19 years and patients who were at least 20 years old (MD=5.833, P<0.05). There was also a positive and significant mean difference between patients who were between the ages of 5 and 19 years and pregnant women (MD=8.833, P<0.05) based on the category of patients who were treated and discharged in relation to malaria infection. The results also showed that in terms of hospitalizations which were not related to malaria infection, children below the age of five were again found to be more vulnerable when compared to pregnant women (MD=5.600, P<0.05) and patients who are at least 20 years old (MD=5.125, P<0.05). The study advocated for reforms that grant free treatment to children below the age of five years since they were found to be the most vulnerable in contracting malaria and non-malaria related diseases and the most vulnerable to hospitalization.
Keywords: Hospitalization, Multivariate Analysis, Statistical Analysis, Clinic data, Malaria
Cite this paper: Bosson-Amedenu Senyefia, Vivian Nimoh, Osei-Asibey Eunice, Statistical Analysis of Trends of Malaria Diagnosis and Patient Demographics: A Multivariate Study of Clinic Data in Ghana, American Journal of Computational and Applied Mathematics , Vol. 9 No. 2, 2019, pp. 43-49. doi: 10.5923/j.ajcam.20190902.03.
Article Outline
1. Introduction
- Malaria remains a devastating public health menace in terms of morbidity and mortality in third world countries. It also remains the main cause of hospitalization and records the highest level of cases in outpatient department [1]. Prevalence of malaria intensity has been in its ascendency often resulting in maternal and infant morbidity and mortality. Pregnant women in sub-Sahara Africa often are in the records of pregnancy-associated malaria, and have been found to have lower immune system compared to non-pregnant women. In spite of the intervention of malaria prevention and control measures such as vector control with insecticide-treated nets (ITNs), indoor residual praying (IRS), intermittent preventive treatment of malaria in pregnancy (IPTp) and effective treatment, Artemisinin based combination therapy (ACT); malaria still remains a serious problem in Africa. Free or subsidized distribution of these control measures have increased from 30% to 100% across Africa and the distribution of bed net is now linked to antenatal care [2]. Approximately 80% of world infection due to malaria is associated with Africa. Out of this percentage, 89% of deaths were found to have occurred in Africa in the year 2008. Malaria prevalence his linked to poverty, ignorance and underdevelopment. In endemic areas of malaria infection, the most group associated with morbidity and mortality is young children, followed by pregnant women. Children under five years are estimated to be the most vulnerable with respect to malaria infection [3].Malaria prevalence has been significantly attributed to Africa and Asia. About 51 percent of all malaria cases worldwide have been attributed to Africa with 42 percent being attributed to Asia. Children below the age of five years have been the most vulnerable group in all malaria patient categories. The malaria mortality of children below the age of five years have been estimated to be more than ten times the rate in industrialized nations [4, 5, 6, 7].Thirteen children below the age of five years have been estimated to die every minute worldwide. Malaria mortality among children below the age of five has been attributed to several risk factors including poverty [8, 9, 10]. The malaria disease accounts for over 61% of hospital admissions as well as 25% rate of mortality of under-five children in Ghana. The disease remains a major threat to the survival of young children in Ghana and the rest of the sub Saharan Africa [11]. To this end; it is prudent to study more into hospital data to be abreast with the current trends in hospital diagnosis with respect to malaria infection in comparison with the various categories of patients including children under five years.
2. Review of Related Literature
- Multivariate analysis procedure has been applied in diverse fields. It was used to study the factors that are linked with the risk of cancer in systemic lupus erythematous (SLE), in relation to a population of 16,409 participants. Cancer diagnosis was confirmed by checking with registry. The findings demonstrated smaller levels of SIR for overall cancer risk within black and white SLE patients. Cancer risk was found to have increased in SLE patients in comparison to the entire population. This was more prevalent with patients of white race and younger patients as well as those with lower SLE span [12]. Another study applied multivariate analysis to a data on pregnant women who visit antenatal clinics or who are hospitalized for non-obstetric connected ailment. Multivariate analysis of antenatal cohorts who domiciled in the district of Bastar known for stable malaria transmission was found to have a strong association with peripheral parasitaemia. Other explanatory variables which were found to be moderately associated were moderate anaemia, fever lasting for one week and lack of formal education. Also similar analysis showed that delivery unit’s participants have strong association with peripheral and/or placenta parasitaemia. Admissions which were linked with malaria were more dominating among pregnant women in Bastar, a district known for high level of malaria prevalence [13].Again, yet another study investigated the prevalence of malaria infection and prevailing risk factors in Sudan. The study interviewed selected sample of 836 pregnant women and examined them for malaria parasite. The multivariate analysis of the data concluded among many others that mothers who were below the age of 20 years as well as those with first and second pregnancies were independent predictors of malaria infection. Also, low-income and illiteracy were also identified as independent predictors. The study also found evidence of good correlation among pregnant women and their socioeconomic status as well as young age [2].Multivariate study was conducted on a group of international travelers who had visited countries within a period of two years. The study examined the health status of the travelers after they reported back to their own countries. The results revealed that the prevalence of travel related diseases was higher among certain subgroups of travelers [14].Yet another study sought to examine the YF vaccination coverage among French travelers who were suspected to be infected by YF virus while in Senegal. The study also sought to determine the factors that had association with vaccination coverage. The study collected responses from respondents on their attitude to YF vaccination before their travels. Multivariate analysis was employed in the determination of factors associated with coverage of vaccination. The study found that over 60% of travelers to Senegal failed to be YF vaccinated before embarking on trip. It was established that YF coverage was influenced by how much they knew about YF and perception of risk about YF in addition to the type of counseling they received before their trip [15].
3. Method
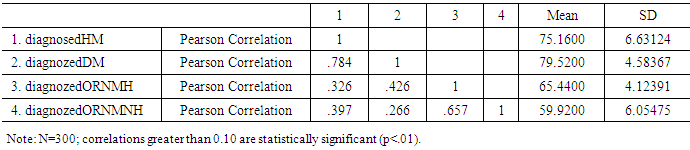
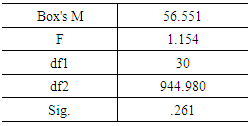
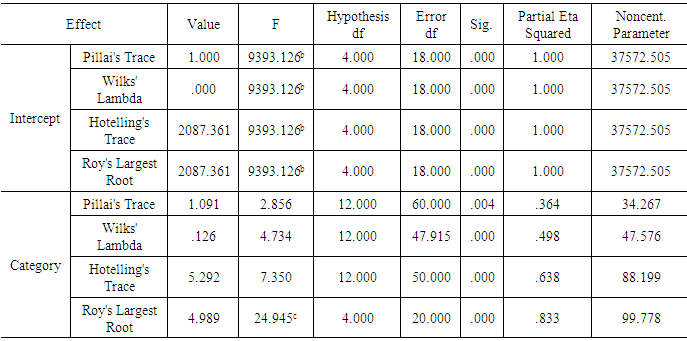
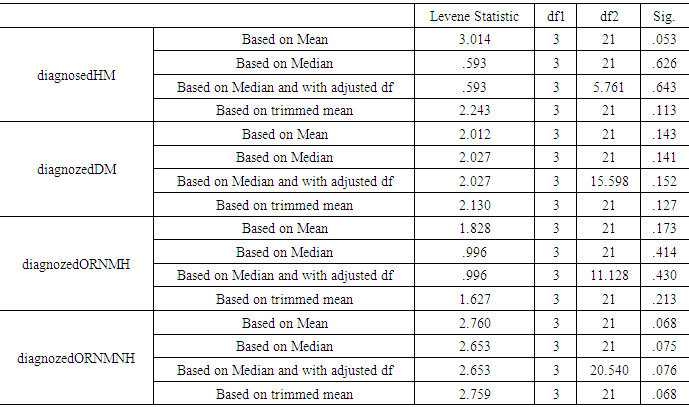
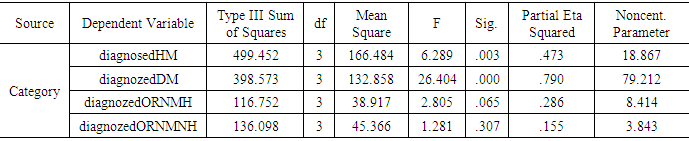
- The study used retrospective hospital data from erstwhile Mpohor district clinic which is the only main clinic that serves all the sub districts (apart from CHIPPS compounds) in that particular district of Ghana. Patients from communities such as Manso, Edum Banso, Mpohor, and Ayiem among others patronize this clinic which in real terms happens to be the biggest health Centre in the district. Multivariate analysis was applied to the data in order to study into the various categories of patients who visit the health Centre. The categories included children less than five years, pregnant women, and people in the age range of 5 to 10 years; and those who are 20 years and above. The study analyzed into the categories of diagnosis resulting in hospitalization due to malaria, hospitalization due to others reason other than malaria, treatment and discharge due to malaria and treatment and discharge due to other illness not having to do with malaria. Pearson’s’ correlations among dependent variables was tested for meaningful pattern within a moderate range, to ascertain the appropriateness of MANOVA procedure. The Box’s M p -value was examined for equality among covariance matrices. A one-way MANOVA was carried out to test the hypothesis that there would be one or more mean differences between patient levels and the diagnosis levels. The homogeneity of variance assumption was tested after performing series of Levene’s F tests. A series of one-way ANOVAs (Tukey was performed for each dependent variable to examine their significance and effect sizes. The post hoc test (Tukey’s test) was employed to check the mean difference between significant categories.
4. Analysis
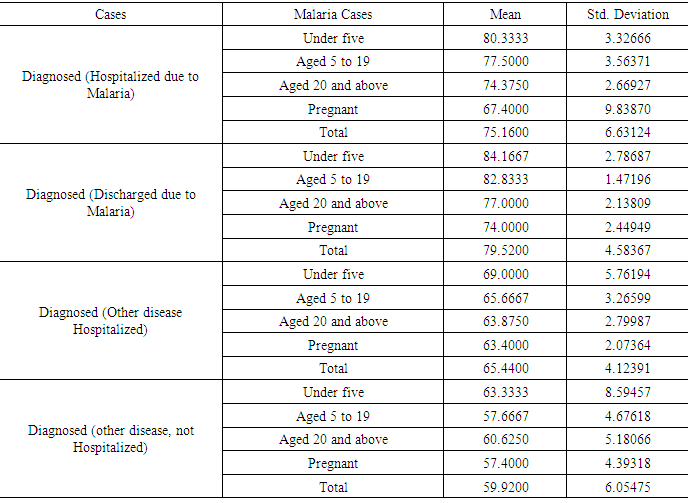
- Table 1 shows the mean and standard deviations of the various categories. It can be seen that the standard deviations of each group is in a range of not more than four times each other, a situation which suggests homogeneity of variance. In general, pregnant women had the lowest mean with children under five having the highest mean across the categories. The general trend is that children under five are more prone to hospitalization and other diseases followed by people aged between 5 and 19. The trend also shows people aged 20 and above are more vulnerable to hospitalization due to malaria and other causes than pregnant patients.
|
|
|
|
|
|
|
5. Conclusions
- Multivariate analysis was applied to hospital data in this study. The underlying assumptions were verified with the data and were satisfied. The results from the post hoc test showed a positive and significant mean difference between children below the age of five years and patients between the ages of 5 and 19 years (MD=3.333, P<0.05). This means children below the age of five are more vulnerable and prone to hospitalization resulting from malaria infection than patients between the ages of 5 and 19 years. Similarly, there was a positive and significant mean difference (MD=12.933, P<0.05) between children below the age five years and pregnant women. This finding means that once again, children below the age of five are more vulnerable and prone to hospitalization resulting from malaria infection than pregnant women. Also, there was a positive mean difference between patients who were at least 20 years old and pregnant women (MD=10.100, P<0.05) when compared on the basis of hospitalization. This indicated that patients who are at least 20 years old are hospitalized more than pregnant women. With reference to the category of patients who were treated and discharged as a result of malaria infection, there was a positive and significant mean difference between patients who are between the ages of 5 and 19 years and patients who are at least 20 years old (MD=5.833, P<0.05). There was also a positive and significant mean difference between patients who are between the ages of 5 and 19 years and pregnant women (MD=8.833, P<0.05) based on the category of patients who were treated and discharged in relation to malaria infection. The results also showed that in terms of hospitalizations which were not related to malaria infection, children below the age of five were again found to be more vulnerable when compared to pregnant women (MD=5.600, P<0.05) and patients who are at least 20 years old (MD=5.125, P<0.05). The study advocated for reforms that grant free treatment to children below the age of five years since they were found to be the most vulnerable in contracting malaria and non-malaria related diseases and the most vulnerable to hospitalization.
6. Recommendations
- The study advocated for reforms to grant free treatment to children below the age of five years since they were found to be the most vulnerable in contracting malaria and non-malaria related diseases; the most vulnerable to hospitalization.