| [1] | International Diabetes Federation, “IDF Diabetes Atlas,” 6th Edn. Brussels, Belgium: International Diabetes Federation (2013). http://www.idf.org/diabetesatlas. |
| [2] | P. J. Watkins, Ed., “ABC of Diabetes”, 5th ed., London: BMJ Books, 2003. |
| [3] | http://diabetes.webmd.com/. |
| [4] | Tuchin V.V, Ed., “Handbook of Optical Sensing of Glucose in Biological Fluids and Tissues”. 1st Edn., CRC Press, Taylor & Francis Group, London, 2009. |
| [5] | A. Tura, A. Maran and G. Pacini, “Non-invasive glucose monitoring: Assessment of technologies and devices according to quantitative criteria”, Diabetes Research and Clinical Practice, vol. 77, pp.16-40, 2007. |
| [6] | “Special issue on non-invasive glucose monitoring with optical technique”, IEEE Leos Newsletter, April, 1998. |
| [7] | J. Tenhunen, H. Kopola, and R. Myllyla, “Non-invasive glucose measurement based on selective near infrared absorption: requirements on instrumentation and special range,” Measurement, vol.24, pp.173–177, 1998. |
| [8] | J.S. Maier, S.A. Walker, S. Fantini, M.A. Franceschini, and E. Gratton, “Possible correlation between blood glucose concentration and the reduced scattering coefficient of tissues in the near infrared,” Opt. Lett., vol. 19, pp.2062–2064, 1994. |
| [9] | A.M.K. Enejder, T.G. Scecina, J. Oh, M. Hunter, W.-C. Shih, S. Sasic, G.L. Horowitz, and M. S. Feld, “Raman spectroscopy for noninvasive glucose measurements,” J. Biomed. Opt., vol. 10, 2005, 031114. |
| [10] | O.S. Abdalsalam, A.A. Awouda, “Noninvasive glucose monitoring using scattering spectroscopy”, American Journal of Biomedical Engineering vol.4(3), pp.53-59, 2014. |
| [11] | J. Lakowicz and B. Maliwal, “Optical sensing of glucose using phase modulation fluorimetry,” Anal.Chim.Acta, vol.271, pp.155–164, 1993. |
| [12] | S. Bockle, L. Rovati, and R.R. Ansari, “Polarimetric glucose sensing using the Brewster-reflection off-eye lens: theoretical analysis,” Proc. SPIE, vol. 4624, pp.160–164, 2002. |
| [13] | C. Chou, C.Y. Han, W.C. Kuo, Y.C. Huang, C.M. Feng, and J.C. Shyu, “Noninvasive glucose monitoring in vivo with an optical heterodyne polarimeter,” Appl. Opt., Vol. 37, pp. 3553–3557, 1998. |
| [14] | S. Yeh, C. F. Hanna, S. Kantor, et al., “Differences in thermal optical response between intact diabetic and nondiabetic human skin,” Proc. SPIE, vol.4958, pp. 213–224, 2003. |
| [15] | Z. Zhao, “Pulsed Photoacoustic Techniques and Glucose Determination in Human Blood and Tissue”, Doctoral Thesis, University of Oulu, Finland, 2002. |
| [16] | K.V. Larin, M.S. Eledrisi, M. Motamedi, R.O. Esenaliev, “Noninvasive blood glucose monitoring with optical coherence tomography: a pilot study in human subjects,” Diabetes Care, vol. 25, no. 12, pp. 2263–2267, 2002. |
| [17] | Orna Amir et al. “Continuous noninvasive glucose monitoring technology based on Occlusion spectroscopy," Journal of Diabetes Science and Technology, vol.1 (4), July, 2007. |
| [18] | H.S. Ashton, H.A. MacKenzie, P. Rae, Y.C. Shen, S. Spiers, et al., “Blood glucose measurements by photoacoustics,” CP463 Photoacoustic and Photothermal Phenomena: 10th International Conference, pp. 570–572, 1999. |
| [19] | L. Zhu, J. Lin, B. Lin, H. Li., “Noninvasive blood glucose measurement by ultrasound-modulated optical technique”, Chinese Optical Letters, vol.11(2), pp.021701-1 to 021701-5, 2013. |
| [20] | O. Khalil, “Noninvasive glucose measurement technologies: an update from 1999 to the dawn of the new Millenium,” Diabetes Technol. Ther., vol. 6, no. 5, pp. 660–697, 2004. |
| [21] | Md. K. Chowdhury, A. Srivastava, N. Sharma, S. Sharma, “Challenges & Countermeasures in Optical Noninvasive Blood Glucose Detection”, International Journal of Innovative Research in Science, Engineering and Technology (IJIRSET), vol.2, issue 1, Jan., pp.324-329, 2013. |
| [22] | A. Srivastava, Md. K. Chowdhury, S. Sharma, N. Sharma, “Blood Glucose Monitoring Using Non Invasive Optical Method: Design Limitations and Challenges”, International Journal of Advanced Research in Electrical, Electronics and Instrumentation Engineering (IJAREEIE), Vol. 2, issue 1, Jan., pp.615-620, 2013. |
| [23] | T. Haar, and S.J. Wyard, “Blood cell banding in ultrasonic standing wave fields: A physical analysis”, Ultrasound in Medicine and Biology, vol. 4(2), pp.111-123, 1978. |
| [24] | Md. K. Chowdhury, A. Srivastava, S. Sharma, N. Sharma, “The potential application of amplitude modulated ultrasound with Infrared Technique for blood glucose level determination in non invasive manner”. Biomedical and Pharmacology Journal, Vol.7, No.1, page no.195-206. (2014). |
| [25] | Md. K. Chowdhury, A. Srivastava, S. Sharma, N. Sharma, “Five days daily sessions of noninvasive blood glucose level predictions based on amplitude modulated ultrasound and infrared technique over a healthy and diabetic subject”. IOSR-Journal of Electrical and Electronics Engineering, Vol.5.Ver. IV, pp-34-41, Sep-Oct.,2014. |
| [26] | S. Radel, M. Brandstetter, B. Lendl, “Observation of particles manipulated by ultrasound in close proximity to a cone-shaped infrared spectroscopy probe”, Ultrasonics, vol. 50, pp.240–246, 2011. |
| [27] | W. T. Coakley, “Ultrasonic separations in analytical biotechnology”, Trends in Biotechnology, pp. 506-511, 1997. |
| [28] | L.V. King, “On the acoustic radiation pressure on spheres”, Proceedings of the Royal Society of London pp.212–240, A147, 1934. |
| [29] | K. Yosioka, Y. Kawasima, “Acoustic radiation pressure on a compressible sphere”, Acustica, vol. 5, pp.167–173, 1955. |
| [30] | F. Petersson, A. Nilsson, C. Holm, H. Jonsson and T. Laurella, “Separation of lipids from blood utilizing ultrasonic standing waves in microfluidic channels”, The Analyst, The Royal Society of Chemistry, vol.129, pp.938-943, 2004. |
| [31] | Md. K. Chowdhury, A. Srivastava, N. Sharma, S. Sharma, “The influence of blood glucose level upon the transport of light in diabetic and non-diabetic subjects”. International Journal of Biomedical and Advance Research, vol.4 (5), pp.306-316, 2013. |
| [32] | A. Srivastava, Md. K. Chowdhury, S. Sharma, N. Sharma, “Optical Clearance Effect Determination of Glucose by near Infrared Technique: An Experimental Study using An Intralipid Based Tissue Phantom”, International Journal of Advances in Engineering & Technology (IJAET), Vol. 6 Issue 3, pp. 1097-1108, July, 2013. |
| [33] | K. Konig, “Multiphoton microscopy in life sciences”, Journal of Microscopy, vol. 200-2, pp. 83-104, 2000. |
| [34] | J. Tenhunen, H. Kopola, and R. Myllyla, “Non-invasive glucose measurement based on selective near infrared absorption: requirements on instrumentation and special range,” Measurement, vol. 24, pp. 173–177, 1998. |
| [35] | O.W. Assendelft, Spectrophotometry of Hemoglobin Derivates, Royal Vangorcum Ltd., Assen, 1970. |
| [36] | Y. Mendelson, “Pulse oximetry: theory and applications for noninvasive monitoring,” Clin. Chem., vol. 38, pp.1601–1607, 1992. |
| [37] | D. J. Cox, W. L. Clarke, L. G. Frederick, S. Pohl, C. Hoover, A. Snyder, L. Zimbelman, W. R. Carter, S. Bobbitt, and J. Pennebaker, “Accuracy of perceiving blood glucose in IDDM”, Diabetes Care, vol. 8, no.6, pp. 529–536, 1985. |
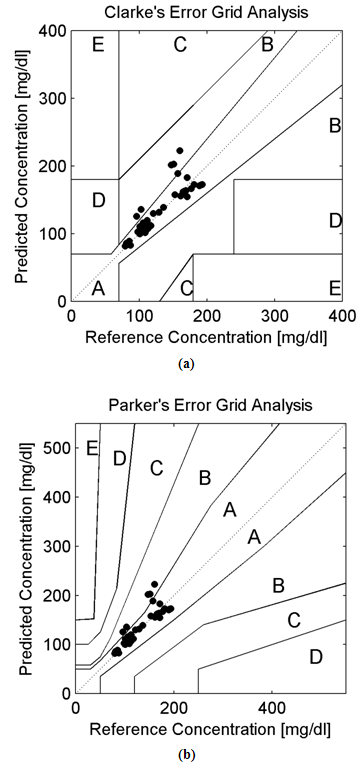
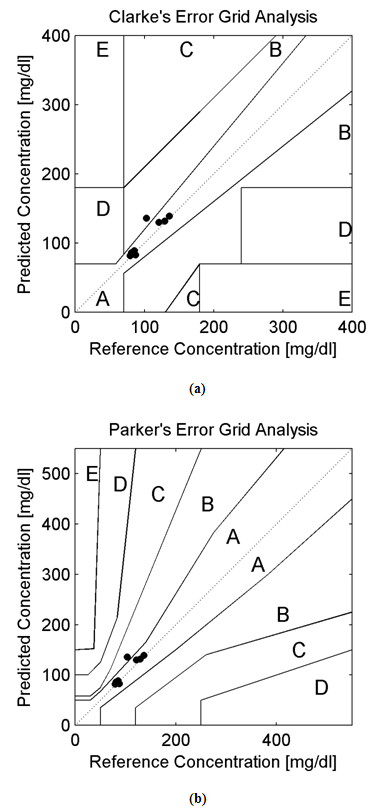
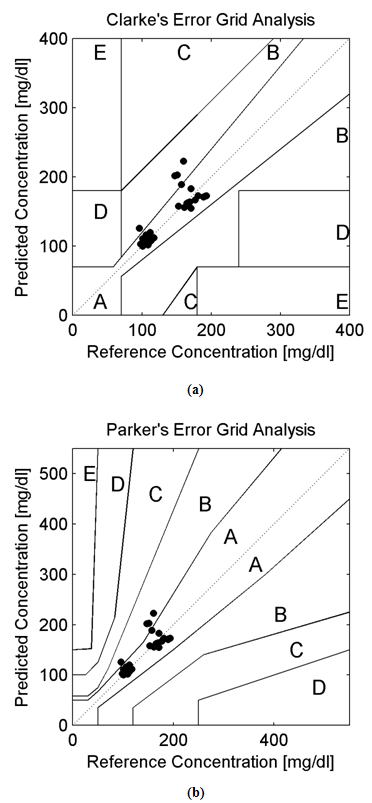
| [38] | W. L. Clarke, L. A. G. Frederick, W. Carter, and S. L. Pohl, “Evaluating clinical accuracy of systems for self-monitoring of blood glucose”, Diabetes Care, vol. 10, no. 5, pp. 622–628, 1987. |
| [39] | A. Maran et al. “Continuous Subcutaneous Glucose Monitoring in Diabetic Patients”, Diabetes Care, Volume 25, Number 2, February, 2002. |
| [40] | B.P. Kovatchev et al. “Evaluating the Accuracy of Continuous Glucose Monitoring Sensors”, Diabetes Care, Volume 27, Number 8, August, 2004. |
| [41] | E. Guevara and F. J. Gonzalez, “Prediction of Glucose Concentration by Impedance Phase Measurements”, in Medical Physics: Tenth Mexican Symposium on Medical Physics, Mexico City (Mexico), vol. 1032, pp.259-261, 2008. |
| [42] | E. Guevara and F. J. Gonzalez, “Joint optical-electrical technique for noninvasive glucose monitoring”, Revista Mexicana De Fisica, vol. 56, no. 5, pp. 430-434, Sep., 2010. |
| [43] | Parkes JL, Slatin SL, Pardo S, Ginsberg BH, “A new consensus error grid to evaluate the clinical significance of inaccuracies in the measurement of blood glucose”, Diabetes Care, vol. 23(8), pp.1143–1148, 2000. |
| [44] | A. Pfutzner, D.C Klonoff, P Scott, J.L Parkes, “Technical Aspects of the Parkes Error Grid”, Journal of Diabetes Science and Technology, vol.7(5), pp.1275-1281, 2013. |
| [45] | J. I Hidalgo, M. J Colmenar, J. L.Risco-M., E. Maqueda, M Botella, J.A Rubio, A.C. Infante, O Garnica, J Lanchares, 2014,“Clarke and Parkes error grid analysis of diabetic glucose models obtained with evolutionary computation”, In Proc., of the 2014 Conf. Companion on Genetic and Evolutionary Computation Companion (GECCO Comp '14). ACM, New York, NY, USA, 1305-1312. |
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML

 ,
,  , (z), (P0), and () stands for radiation force characteristics, volume of the respective molecules, space form the node of pressure, ultrasonic wave peak amplitude and wavelength of ultrasound respectively [23-32].When compressibility aspects
, (z), (P0), and () stands for radiation force characteristics, volume of the respective molecules, space form the node of pressure, ultrasonic wave peak amplitude and wavelength of ultrasound respectively [23-32].When compressibility aspects  of the suspending (blood tissue complex) segment present in human volunteers finger are considered, the mathematical expression had been represented as given below:
of the suspending (blood tissue complex) segment present in human volunteers finger are considered, the mathematical expression had been represented as given below:
 stands for compressibility of the molecules and
stands for compressibility of the molecules and  ,
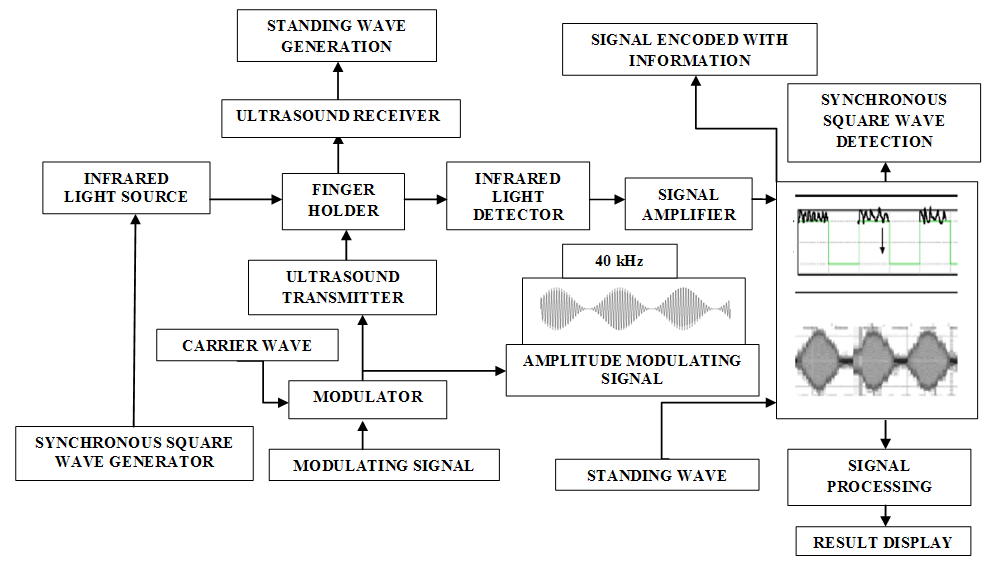
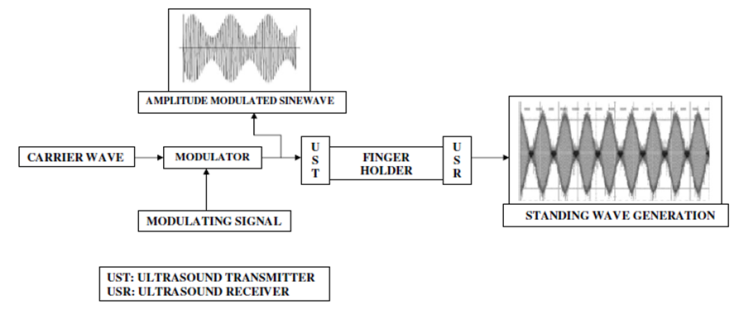
,  signifies molecular density of the suspending molecules and suspending segment respectively [23-32].When infrared light beam propagates through these ultrasound (amplitude modulated ultrasonic waves) excited (blood tissue complex) optical medium, the glucose molecule vibration specific signatures are captured by the respective IR sensitive detectors. This light interaction phenomenon had been represented by Beer-Lambert Law [23-32] as follows:
signifies molecular density of the suspending molecules and suspending segment respectively [23-32].When infrared light beam propagates through these ultrasound (amplitude modulated ultrasonic waves) excited (blood tissue complex) optical medium, the glucose molecule vibration specific signatures are captured by the respective IR sensitive detectors. This light interaction phenomenon had been represented by Beer-Lambert Law [23-32] as follows: