-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Biochemistry
p-ISSN: 2163-3010 e-ISSN: 2163-3029
2025; 15(2): 25-31
doi:10.5923/j.ajb.20251502.01
Received: May 11, 2025; Accepted: Jun. 3, 2025; Published: Jun. 13, 2025

Vitamins A and D Deficiency Among Some Type 2 Diabetics HIV Seropositive Patients Followed in Antidiabetic Center of Abidjan, Ivory Coast
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAïssé Florence Judith Trebissou1, Passi Alice Nzambi Epouse Matété Mounoi1, 2, Adou Francis Yapo2
1Biology Laboratory and Medical Research, National Institute of Public Health, Abidjan, Ivory Coast
2Pharmacodynamics-Biochemistry Laboratory, UFR Biosciences, Félix Houphouët Boigny University, Abidjan, Ivory Coast
Correspondence to: Aïssé Florence Judith Trebissou, Biology Laboratory and Medical Research, National Institute of Public Health, Abidjan, Ivory Coast.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The Human Immunodeficiency Virus (HIV) is characterized by a cytopathogenicity and a high faculty to provoke some slow and severe infections. To immune system perturbations, it has come to add some metabolic troubles in the persons living with HIV. The study aims to explore the levels of vitamins A and D in the type 2 diabetics patients infected by HIV and followed at the antidiabetic center of Abidjan. The study population constituted of type 2 diabetics HIV seropositive patients, as some controls without diabetes and HIV. They were eighteen (18) years and older. Vitamins A and D dosages were realized with the High Performance liquid chromatography chain (HPLC). In total 250 people were included in our study. There were 100 type 2 diabetics HIV seropositive patients (T2D/HIV+) and 150 controls. In the study population, women were more than represented with 63% and men 37%, so be it a ratio sex of 0.6. 73% of diabetics infected by HIV presented a deficiency of vitamin A and 27% had some normal rates. 100% of T2D/VIH+ had a deficiency in vitamin D. The dosages of vitamins A and D are very important and should be integrated in the medical care of T2D/HIV in favouring a supplementation in vitamins A and D in these patients.
Keywords: Vitamins A and D, Type 2 diabetes and HIV/AIDS co-infection, Ivory Coast
Cite this paper: Aïssé Florence Judith Trebissou, Passi Alice Nzambi Epouse Matété Mounoi, Adou Francis Yapo, Vitamins A and D Deficiency Among Some Type 2 Diabetics HIV Seropositive Patients Followed in Antidiabetic Center of Abidjan, Ivory Coast, American Journal of Biochemistry, Vol. 15 No. 2, 2025, pp. 25-31. doi: 10.5923/j.ajb.20251502.01.
Article Outline
1. Introduction
- Human immunodeficiency virus (HIV) is characterized by cytopathogenicity and a great faculty to provoke some slow and severe infections. To immune system perturbations, it has come to add some metabolic troubles in the persons living with HIV [1]. These troubles increase significantly the risk of cardiovascular diseases and of type 2 diabetes [2]. While the mortality due to AIDS in terminal phase decreased, type 2 diabetes mellitus and complications appeared as one of the important causes of morbidities and mortalities in the population infected by HIV [3].Diabetes mellitus is oneself an ordinary affection with an important morbidity associated [4]. It to characterized so be it by chronic hyperglycemia, so be it a fasting glycemia superior at 1.26 g/l (7 mmol/L) at least at two resumptions [5]. The estimations of the International Federation of Diabetes (IFD) of 2017 indicate that nearly half a billion people suffer at present from diabetes in the world [6]. In accordance with the datas of National Program of Prevention of Non Transmissible Diseases (NPPNTD), the prevalence of diabetes in Côte d’Ivoire is of 6.2 in 2019 [7].Diabetes mellitus (DM) remains a global health challenge, necessitating the exploration of novel therapeutic strategies. Dipeptidyl Peptidase-4 (DPP-4) inhibitors have emerged as effective treatments by enhancing incretin-mediated insulin secretion. [8] investigated bioactive compounds from three African plants, Ocimum gratissimum, Colocasia esculenta L., and Jatropha curcas L, as potential DPP-4 inhibitors through an integrative computational approach. Authors conclude that the current computer-aided modeling showed that daidzein and salvigenin might have the potential to inhibit DPP-4 activity in diabetes mellitus. Also, antioxidants are chemical compounds that may protect cells from the damage caused by unstable molecules known as free radicals. [9], On the basis of the combination principles, they have designed and synthesized, in very good to excellent yields, a novel series of 5-substituted-2-(3,4,5-trihydroxyphenyl)-1,3,4-oxadiazole compounds (compounds 3n-z) in which a bioactive aromatic 1,3,4-oxadiazole ring is directly linked with an antioxidant 3,4,5-trihydroxyphenyl moiety and an aiding substituent at the two carbons of the ring, the produced 2,5-disubstituted-1,3,4-oxadiazoles were characterized by most different spectral and elemental analytical methods. They found excellent antioxidants, compounds 3s, u, w. [10] showed that three compounds 3b, d, h, exhibited interestingly very high antioxidant activities and they could be very promising lead and parent compounds for the design and synthesis of new antioxidant agents by further in vivo biological evaluation, structural modifications, investigations, computational studies. However [11], brought that the HIV infection and the antiretrovirals Treatments are purveyors of insulinoresistance and the diabetes. This is the case of protease inhibitors that carry some perturbations of lipid metabolism and of carbohydrate abnormalities, among others an insulinoresistance, in the base of diabetes. This induces then some biochemical, haematological and an oxidative stress perturbations [12]. This is the case of vitamins that are of necessary substances at the growth and at the good functioning of the organism, that produces insufficient quantity for themselves needs (vitamins B6, F, K, PP) or not can them synthesize and are brought by food [13]. Palmitic or hexadecanoic acid is one of the most plentiful and widespread saturated fatty acids present in almost all living creatures. Pharmacologically, palmitic acid and its esters/salts have many clinical applications in humans, retinyl palmitate ester is known to be a major source of vitamin A, ascorbyl palmitate compound is a fat-soluble ester form of the important water-soluble L-ascorbic acid vitamin C and it is also employed as an antioxidant food additive [14]. Indeed, some authors have reported deficiencies in vitamin A in the patients infected by the HIV [15]. Too, the balance of vitamins in the organism could be disrupted during the co-infection HIV/AIDS and type 2 diabetes. It is in this perspective that this study was realized and whose general objective is to explore the levels of vitamins A and D in type 2 diabetics patients infected by HIV and followed at Antidiabetics Center of Abidjan.
2. Material and Methods
- This study has been validated by the National Committee of Ethics of Sciences of the Life and the Health of Côte d’Ivoire in accordance with N/Ref: 163-18/MSHP/CNESVS-km of 15th January 2019.Type and Context of studyThis is a Cross-sectional study which took place from January 2021 to 2022 in Antidiabetics Center of Abidjan.The Antidiabetics Center of Abidjan is a center of health located within the National Institute of Public Health of Côte d’Ivoire. It oversees medical care for patients suffering from diabetes. It has many units who’s that is of medical care of diabetics living with HIV/AIDS patients.Study populationThe study population was constituted of type 2 diabetics HIV seropositive patients. These patients were aged 18 years and older. The parents who supported patients and who did not present either diabetes or HIV have constituted control of population. These patients have permitted to constitute three groups:- Group 1 = Co-infection Type 2 Diabetics HIV-1 seropositive (T2D/HIV-1+).- Group 2 = Co-infection Type 2 Diabetics HIV-2 seropositive (T2D/HIV-2+).- Group 3 = Control without diabetes nor HIV.Inclusion criteria- All type 2 diabetics HIV seropositive patients whose the age was higher 18 years old than or egal.- All parents of patients not hading neither diabetes nor HIV and aged of 18 years and older.- To give his consent to participate to the study.Non-inclusion criteriaNo have participated to the study, the pregnancy women, type 1 diabetics and the persons no having consented at the study.Exclusion criteriaThe control population recruited and whose the HIV seropositivity was discovered subsequently, have been excluded from the study.Recruitment of the patientsThe preselection of patients was carried out from the analysis of medical records. The patients reserved were contacted by phone for an appointment to Biology Laboratory of Medical Research (BLMR) of National Institute of Public Health. On the day of appointment, the patients were welcomed to reception service of BLMR and were informed of the study. The sheet of consent was presented to patients to obtain their agreement to participate in the study. The control population were the parents of patients. A blood sample was taken at an elbow crease on a red tube.Dosage of vitamins A and DThe dosage of vitamins A and D were realized with the High Performance liquid chromatography chain (HPLC) in accordance with the methods of [16,17].1. Principle of the high performance liquid chromatography chainTo realize the separation of the mixture, it is diluted into an appropriate solvent, then we inject a volume restrained into chromatochraphic system through the buckle of injection. The compounds of the mixture are transported by the moving phase in which they are soluble, toward the column, seat of the stationary phase. Under the influence of both antagonistic effects of which the driving effect trained by the moving phase and the effect of retention trained by the stationary phase, the constituent of the mixture to move at of different speeds and are separated. This separation is based on the difference of affinity of compounds of mixture opposite the stationary phase, the constituent which has more affinity will be more than restrained. At level of the detector, each compound of mixture outgoing of the column is detected by a signal then it is registered by the system of the treatment of datas under form of a peak. Together of peaks form a chromatogram. 2. Preparation of standardsThe standards (purity > 95%) were diluted into the ethanol to obtain mother solutions at 10 mg/mL for the vitamins A, D and the retinyl acetate. For these solutions, 0.003 mg of standard (vitamin A, D and the retinyl acetate) has been mixed with 3 ml of ethanol. The solutions were prepared into amber tubes to protect the molecules of light. These solutions were prepared by dissolution into the ethanol of the weighed quantity to obtain a concentration of 10 mg/ml. These solutions were then homogenized to the vortex then conserved at 20°C until use.Each standard solution was ejected so that to determine the time of retention and to get the ultraviolet specters of each compound. The girl’s solutions obtained by dilution of mother solutions in the pure ethanol at 1/10, 1/100, 1/1000, 1/10000 served as a calibration range.3. Preparation of the samplesThe aliquots were defrosted in the refrigerator between 4 and 8°C. The retinyl acetate used as standard served at the extraction of vitamins A and D after having added at the aliquots. At this mixture, ethanol was added for isolation of vitamins then they were extrated by adding of n-hexane. A vigorous mixture at the vortex followed of the centrifugation at 3500 turns/minute at 4°C were carried out. The supernatant was recoved and submissive at evaporation under flux of azote. The dried extract obtained was replaced in suspension in 2000 µL of methanol.4. Chromatographic conditionsAfter the calibration, both vitamins were measured out simultaneously, in isocratic modes with the column of C18 type. The moving phase has been a mixture of methanol-water in the proportions 97: 3 (v/v), with a debit of 1 mL/ minute. The temperature of the column was of 40°C. The detection was carried out with a wavelength of 280 nanometers.The normal values of the vitamin A are of 303 – 676 µg/L and those of the vitamin D of 20 – 60 µg/L. A deficiency in vitamin A to express by the values less than 303 µg/L (< 303 µg/L). The deficiency in vitamin D corresponds to values less than 20 µg/L (< 20 µg/L).Statistical analysis of datasDatas were analized with the softwares Microsoft Excel 365 personal (2025) and Graphpad Prism version 10.4.2 (633) (Dotmatics). P-values, with values less than 0.05 and 0.01, were considered statistically significant.
3. Results
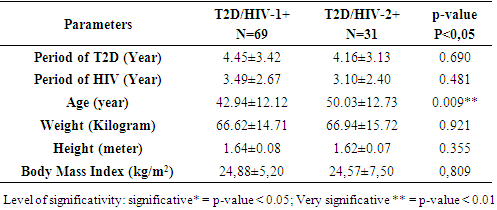
- Sociodemographic and anthropometric characteristics of the study populationIn total 250 people were included in our study. There were 100 type 2 diabetics HIV seropositive patients (T2D/HIV+) and 150 controls. In the study population, women were more than represented with 63% and men 37%, so be it a ration sex of 0.6. There were 69 persons (69%) with HIV-1 type and 31 (31%) persons with HIV-2 (p < 0.05). In the T2D/VIH+, the mean age was 45.14 ± 12.68 years old, whereas at the controls, the mean age was 37.27 ± 13.63 years old. The period of HIV at the T2D/HIV-1+ was 3.49 ± 2.67 years old and 3.10 ± 2.40 years old at the T2D/VIH-2+ (p = 0.481) (table 1).
|
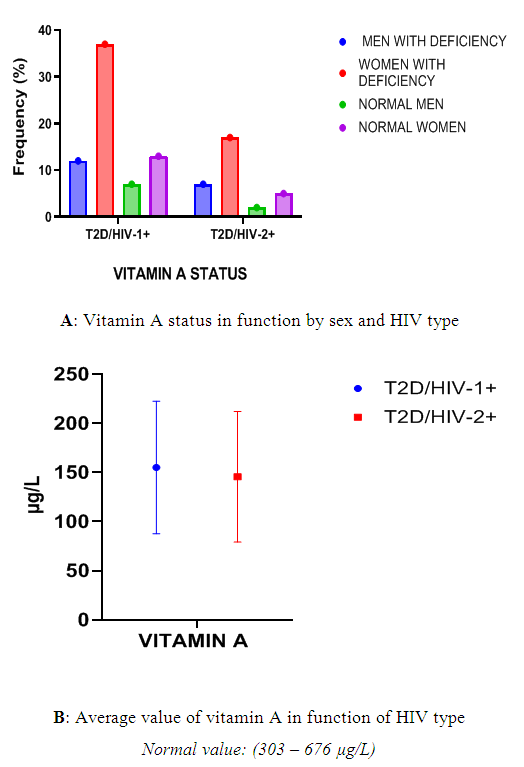 | Figure 1. Vitamin A profile in function of sex and HIV type |
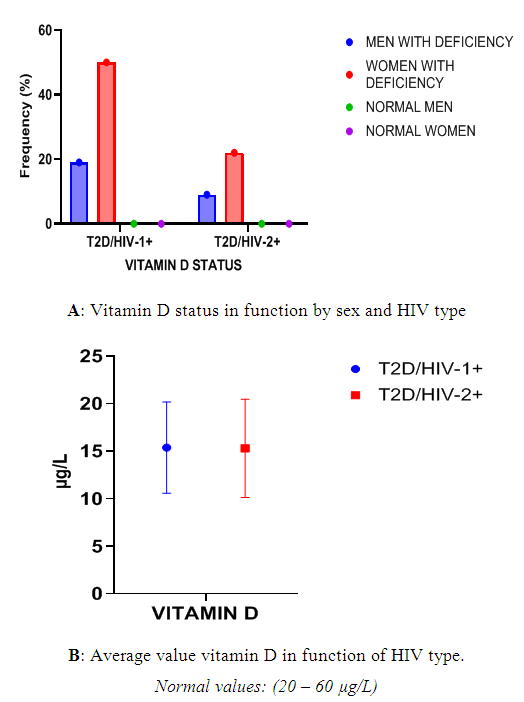 | Figure 2. Vitamin D profile in function of sex and HIV type |
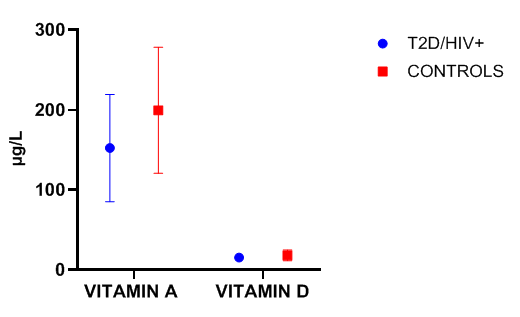 | Figure 3. Average value of vitamins A and D at the T2D/HIV and Control population |
4. Discussion
- Our study aims was to explore the profiles of vitamin A and D at type 2 diabetics patients infected by HIV/AIDS. Our results showed the presence of 100 type 2 diabetics HIV seropositive patients (T2D/VIH+). Indeed, type 2 diabetes is the one of diseases which become more common, particularly in Africa in reason of the speed transition of the life modes [18]. Some recent studies associated type 2 diabetes with the infection by the HIV [19]. Nowadays, several herbal, antioxydant or chemically synthesized medicines are very effective against diabetes [20,21,22,23,24,25,26,27]. According to [28], the combination principles, if three substituted aromatic heterocyclic rings of the three previously mentioned types are directly linked with a citric acid scaffold at the positions of the carboxy groups, the resulting derivatives are expected to be pharmacologically very active. Also, Galloyl hydrazide is a very important and unique organic chemical intermediate with, mainly, antioxidant and anticancer biological activities. [29] maked two standard and fixed methods of synthesis (conventional and greener) of galloyl hydrazide through designing and constructing a new one-pot solventless greener microwave-assisted synthetic method, in addition to redesigning and qualifying the old traditional conventional heating one; both methods are followed by very accurate identification and characterization data, which can be referenced for the efficient reproducibility in the organic and pharmaceutical chemistry community, of galloyl hydrazide.In our study, women T2D/HIV+ were more than represented with 63%. Our results corroborate those of [30], in South Africa who reported 67.76% of type 2 diabetics HIV seropositive women. There was a predominance of HIV-1 in our study as it demonstrated [16].At the level vitaminic profile, three essential points were written by [31] on vitamin A. It is first a potent antioxidant and has the potential to modify the expression of genes. Then, it regulates the liberation of insulin and energy homeostasis. The putative targets of the retinol therapy in type 2 diabetes are the free radicals and the genes implicated in the signs of insulin and obesity. Vitamin A plays an essential role in embryonic development, immunity and the visual cycle [32]. As for vitamin D, it is known and studied for many years for its major role in the phospho-calcic homeostasis which contributes to the development and at balance of bone mineralization. In the context, it evoked a link between vitamin D and type 2 diabetes. Indeed, this vitamin could interact with the different physiopathological mechanism governing the insulinosecretion, the insulinoresistance and the glucidic homeostasis parameters. It could also intervene on the complications of type 2 diabetes [33].In our study, the average values of vitamins A and D were low in all groups in general and particularly in diabetics living with HIV. Our results agree with those of [34], having reported some deficiencies in vitamins A and D in the context of the HIV infection. Insufficient rates in vitamin A have also been reported by [15] in people living with HIV. In diabetics living with HIV of our study, the alteration of HIV immunity could explain these insufficiencies in vitamin A and D. Our results corroborate those of [31] who showed that a deficiency in vitamin A was associated at the diminution of immunity and blindness. Also, in type 2 diabetes, it was demonstrated that vitamin A can regulate the metabolic ways implicated in the pathogenesis of obesity and of diabetes [35]. Moreover, some researchers demonstrated that the seric vitamin A or the contributions in provitamin A carotenoids, such as the β-carotene protect against the resistance at the insulin [36]. Moreover, the work of [37] has shown a primary relation between the supplementation of vitamin A and a decrease of complications associated at the type 2 diabetes. This low rates of vitamin A in diabetics living with HIV could be one of causes of complications.All as vitamin A, the deficiency or the insufficiency of vitamin A could disturb the immune function. Therefore, it could precipitate the destruction of TCD4 lymphocyte and the progression of the HIV desease and the diabetes [38].
5. Conclusions
- Our study aims to explore the level of vitamins A and D in the type 2 diabetics HIV/AIDS seropositive patients. The results show that 73% of T2D/HIV patients had a deficiency in vitamin A and 100% of T2D/HIV+ patients presented a deficiency in vitamin D. Population control also presented a deficiency in vitamin A and D. The clinicians responsible for the medical care of type 2 diabetics HIV seropositive patients must take these deficiencies into the account in favorizing the supplementation in vitamins A and D in these patients.The control population must improve their diet in favorizing the consumption of foods rich in vitamins A and D. Foods of animal origin rich in vitamin A are the liver, eggs, oily fish, whole milk and non-skimmed dairy products (butter, cream). Foods of vegetable origin rich in vitamin A are green, yellow (lemons, grapefruits) or orange (mangoes, oranges, carrots) fruits and vegetables, which contain carotenoids, which transform partially in vitamin A in the organism. Foods more than rich in vitamin D are the liver of lean fish (cod liver oil), oily fish, egg yolk, liver, whole milk and non-skimmed dairy products (especially butter).We recommend at the type 2 diabetics HIV seropositive patients and at the control population to make a checkup of vitamins A and D once a year.
Conflict of Interest
- There is no conflict of interest in our study.
ACKNOWLEDGEMENTS
- We thank AntiDiabetic Center of Abidjan for giving us all patients.