-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Biochemistry
p-ISSN: 2163-3010 e-ISSN: 2163-3029
2024; 14(1): 1-4
doi:10.5923/j.ajb.20241401.01
Received: Jan. 20, 2024; Accepted: Feb. 19, 2024; Published: Mar. 4, 2024

Interest in Measuring Apolipoproteins A1 and B in Type 2 Diabetics
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLNiokhor N. Diouf1, Maimouna Touré2, Ousseynou Boye3, Mame N. Coly1, Moustapha Djité4, Najah F. Coly5, Idrissa Y. Soumah6, Abdourahmane Samba6, Ibrahima Faye6, Fatou Diédhiou6, Souleymane Thiam6, Arame Ndiaye6, Fatou Cissé6, Fatou Diallo6, Maguette Sylla-Niang3, Alassane Diatta1
1Department of Biology and Functional Explorations, Assane Seck University, Ziguinchor, Senegal
2Physiology Laboratory of the Cheikh Anta Diop University, Dakar, Senegal
3Medical Biology Laboratory of Idrissa Pouye General Hospital, Dakar, Senegal
4Pharmaceutical Biochemistry Laboratory of Cheikh Anta Diop University, Dakar, Senegal
5Biochemistry Laboratory of Iba Der Thiam University, Thies, Senegal
6Medical Biochemistry Laboratory of Cheikh Anta Diop University, Dakar, Senegal
Correspondence to: Niokhor N. Diouf, Department of Biology and Functional Explorations, Assane Seck University, Ziguinchor, Senegal.
| Email: |  |
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Objective: To study the routine lipid profile, apolipoprotein A1 and B levels, determine the types of dyslipidemia and their frequency in type 2 diabetic patients. Materials and method: This is a prospective cross-sectional study involving 100 type 2 diabetic patients. Each patient received a routine lipid profile and a dosage of apolipoproteins A1 and B. Results: Increased apolipoprotein B is the most common lipid abnormality occurring in 31% of type 2 diabetic patients. This abnormality is followed by hypertriglyceridemia found in 17% of cases. The low serum HDL cholesterol level is identical to that of the low apolipoprotein A1 level which is 11%. Only 7% of patients have normal triglyceride levels associated with hyperLDL cholesterol compared to 16% who have normal triglycerides with elevated apolipoprotein B levels. 18% of patients have normal LDL cholesterol levels associated with elevated apolipoprotein B levels. High values of the apolipoprotein B/apolipoprotein A1 ratio and those of the LDL cholesterol/HDL cholesterol ratio have a frequency of 24% and 13%, respectively. Apolipoprotein B is significantly higher in women than in men (p=0.003). Total cholesterol and LDL cholesterol were significantly higher in patients with an HbA1c level ≥ 8% compared to those with an HbA1c level < 8% (p=0.02 and p=0.03 respectively). Conclusion: This study shows a high frequency of dyslipidemia. Increased apolipoprotein B is the most common lipid abnormality in type 2 diabetes. Measuring apolipoprotein B and determining the apolipoprotein B/apolipoprotein A1 ratio could be early indicators for predicting cardiovascular risk.
Keywords: Dyslipidemia, Apolipoprotein A1, Apolipoprotein B, Type 2 diabetes mellitus
Cite this paper: Niokhor N. Diouf, Maimouna Touré, Ousseynou Boye, Mame N. Coly, Moustapha Djité, Najah F. Coly, Idrissa Y. Soumah, Abdourahmane Samba, Ibrahima Faye, Fatou Diédhiou, Souleymane Thiam, Arame Ndiaye, Fatou Cissé, Fatou Diallo, Maguette Sylla-Niang, Alassane Diatta, Interest in Measuring Apolipoproteins A1 and B in Type 2 Diabetics, American Journal of Biochemistry, Vol. 14 No. 1, 2024, pp. 1-4. doi: 10.5923/j.ajb.20241401.01.
Article Outline
1. Introduction
- Patients with type 2 diabetes mellitus (T2DM) are at increased risk of cardiovascular disease, which remains the leading cause of morbidity and mortality worldwide and dyslipidemia is the major cardiovascular risk factor in these patients [1]. Apolipoproteins, protein components of lipoproteins, ensure the transport of lipids and the stabilization of the structure of lipoproteins, activate enzymes participating in their metabolism and also recognize endothelial receptors associated with inflammatory signaling pathways [1,2]. They would therefore be associated with the pathophysiological processes of T2DM and apolipoprotein B (apo B) would be superior to LDL cholesterol as a marker of cardiovascular disease. Its dosage in type 2 diabetics, associated with that of apolipoprotein A1 (apo A1), makes it possible to better assess the cardiovascular risk in these patients [3]. Based on this constant, it is therefore judicious to determine apolipoproteins A1 and B and compare them to the routine lipid profile. Thus the objective of this study is to study the routine lipid profile and the levels of apolipoproteins A1 and B, to determine the types of dyslipidemia and their frequency in type 2 diabetic patients.
2. Materials and Method
- We conducted a prospective cross-sectional study which took place over a period of 6 months and involved 100 type 2 diabetics (31 men and 69 women) who presented to the Medical Biology Laboratory of the Idrissa Pouye General Hospital (Dakar, Senegal) for biological monitoring.The patients included in the study were type 2 diabetics received at this laboratory during the study period, who agreed to participate after free and informed consent.Patients with dysthyroidism, liver disease, nephropathy or taking medications likely to affect lipid metabolism were excluded from the study.The type 2 diabetics thus selected were matched according to age and sex and the duration of progression of diabetes was also determined. A venous blood sample taken after a 12-hour fast was used to measure fasting blood glucose, total cholesterol, HDL cholesterol and triglycerides by enzymatic method (Abbott Diagnostics, Sligo, Ireland) and to measure glycated hemoglobin (HbA1c) by immunoturbidimetric method (Abbott Diagnostics, Sligo, Ireland). LDL cholesterol was calculated according to the Friedwald formula when its value was less than 4 g/l [4], otherwise it was measured directly in immunoseparation using latex particles grafted with monoclonal antibodies (Abbott Diagnostics, Sligo, Ireland).The data were entered into Excel 2013, the statistical analysis was carried out using R software version 4.3.1. The mean and standard deviation were calculated and the Student's T-test was used to compare the observed results. A p-value less than 0.05 was considered statistically significant and not significant in other cases.
3. Results
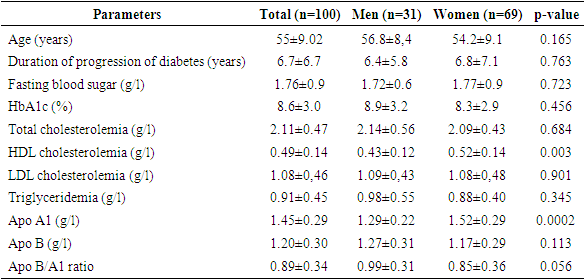
- The study population consists of a total of 100 type 2 diabetic patients characterized by a female predominance with 69% women, an average age of 55 ± 9.02 years and an average duration of diabetes of 6.74 ±6.76 years. The overall prevalence of dyslipidemia is 38%. Increased apolipoprotein B is the most common lipid abnormality occurring in 31% of type 2 diabetic patients. This abnormality is followed by hypertriglyceridemia found in 17% of cases and total cholesterol and serum LDL cholesterol in 14% of cases each. The low serum HDL cholesterol level is identical to that of the low apolipoprotein A1 level which is 11%. Only 7% of patients have normal triglyceride levels associated with hyperLDL cholesterol compared to 16% who have normal triglycerides with elevated apolipoprotein B levels. 18% of patients have normal LDL cholesterol levels associated with elevated apolipoprotein B levels. High values of the apolipoprotein B/apolipoprotein A1 ratio and those of the LDL cholesterol/HDL cholesterol ratio have a frequency of 24% and 13%, respectively. HDL cholesterol and apolipoprotein B as shown in Table 1, are significantly higher in women than in men (p=0.003 and p=0.0002 respectively).
|
|
|
4. Discussion
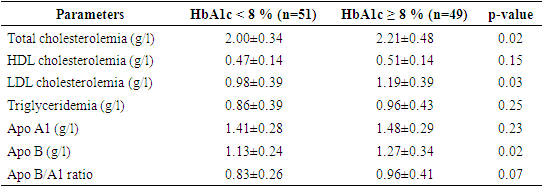
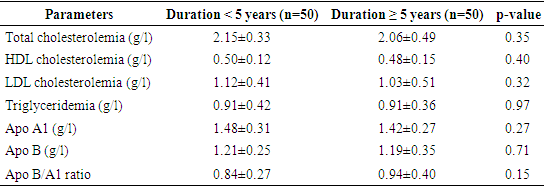
- T2DM is characterized by a set of disorders of carbohydrate metabolism having a common main characteristic, chronic hyperglycemia resulting from defects in insulin secretion, insulin action or the combination of two phenomena [5]. This abnormality of secretion and/or activity of insulin is the cause of anomalies in all species of lipoproteins favoring lipid deposit in the wall of blood vessels and constituting a risk factor and a characteristic sign of atherosclerosis [6]. In our study, 49% of diabetic subjects had poor glycemic control and were therefore likely to present with dyslipidemia. The prevalence of dyslipidemia in our patients is 38%. A Nigerian study and a Somali study, in type 2 diabetics, obtained higher prevalences, respectively 69.3% [7] and 92.8% [8]. Many authors stipulate that dyslipidemia in type 2 diabetic subjects is mainly marked by hypertriglyceridemia and a decrease in serum HDL cholesterol [9,10]. We found isolated dyslipidemia composed of hypertriglyceridemia at 17% and LDL cholesterol at 14%, reflecting a greater frequency of apo B lipoproteins and low HDL cholesterol at 11%. These results are concordant with other studies which also show a preponderance of hypertriglyceridemia, total hypercholesterolemia and increased LDL cholesterol in type 2 diabetics. Thus Bello-Ovosi et al [7] also obtained results similar to ours with a more frequent mixed dyslipidemia composed of a high level of triglycerides and low density lipoprotein cholesterol in 41% of their patients. Alici G et al [8] also confirm our results by presenting a high rate of low density lipoproteins (non-HDL lipoproteins) at 82.8%. This significant increase in apolipoprotein B lipoproteins is due to a combination of excessive fatty acid intake and limited apolipoprotein B degradation explaining the hypertriglyceridemia characteristic of insulin resistance [6,11]. Kanani FH et al. [12] demonstrated that non-HDL cholesterol and apolipoprotein B show a similar tendency in type 2 diabetics with hypertriglyceridemia, but apolipoprotein B identifies other patients at high cardiovascular risk who have normal triglycerides. Some authors suggest, in the biological monitoring of diabetic subjects, the measurement of apolipoprotein B and the determination of the ApoB/A1 ratio which could be early indicators for predicting cardiovascular risk in these patients [13,14]. Elevated apolipoprotein B increases the risk of coronary heart disease and retinopathy, making it essential for these patients to adopt a lifestyle and take treatment aimed at reducing this level to help increase their life expectancy [15,16,17]. Recent data indicate that low serum levels of HDL cholesterol and the functionality of HDL particles, lipoproteins to apoproteins A1, are correlated with the pathogenesis and prognosis of type 2 diabetes mellitus and that it is chronic hyperglycemia that causes this decrease in serum levels and deterioration of their functionality [18]. Our results show higher HDL cholesterol and apolipoprotein A1 values in female subjects, which is in contradiction with the Somali study by Alici G et al. [8] where dyslipidemia marked by low HDL cholesterol is more common in women than men. In some studies, poor glycemic control defined by an HbA1c level greater than or equal to 8% is significantly associated with dyslipidemia in type 2 diabetic patients [19,20]. According to an Indian study, dyslipidemia does not result from poor glycemic control, however the duration of progression of diabetes is significantly associated with poor glycemic control [21]. In our study, total cholesterol and HDL cholesterol levels were significantly higher in patients with poor glycemic control than in those with an HbA1c value strictly below 8%. We did not find a statistically significant difference in the variation of lipid parameters according to the duration of diabetes.
5. Conclusions
- This study shows a high frequency of dyslipidemia. Increased apolipoprotein B is the most common lipid abnormality in type 2 diabetes. It helps identify individuals at high risk of cardiovascular disease who would not otherwise be detected on routine lipid profile. Measuring apolipoprotein B and determining the apolipoprotein B/apolipoprotein A1 ratio could be early indicators for predicting cardiovascular risk.
ACKNOWLEDGEMENTS
- We thank all the staff of the medical biology laboratory of the Idrissa Pouye General Hospital and that of the biochemistry laboratory of the Aristide Ledantec Hospital for their material support. We also thank all patients who agreed to participate in the study.
Conflicts of Interest
- The authors declare that they have no conflict of interest in relation to this article.