-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Biochemistry
p-ISSN: 2163-3010 e-ISSN: 2163-3029
2019; 9(2): 17-20
doi:10.5923/j.ajb.20190902.01

Comparative Study of Lipid Profile in Patients with Chronic Kidney Disease on Haemodialysis / Conservative Management with Control Population
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMuhammed Sanoop A. V.1, Shifa K.2, Vipindas K.3
1Asst Professor, Department of Biochemistry, MES Medical College, Malaparambu, Perinthalmanna, Kerala, India
2Professor and HOD, Department of Biochemistry, MES Medical College, Malaparambu, Perinthalmanna, Kerala, India
3Asst Professor, Mechanical Engineering Department, Deendayal Petroleum University, Gandhinagar, Gujarat, India
Correspondence to: Muhammed Sanoop A. V., Asst Professor, Department of Biochemistry, MES Medical College, Malaparambu, Perinthalmanna, Kerala, India.
| Email: |  |
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

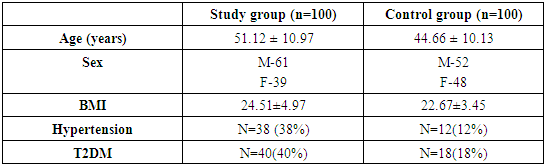
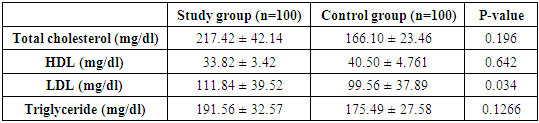
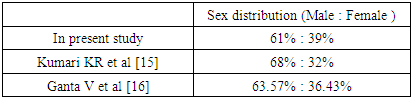
Chronic renal failure has increased in incidence and requirement of renal replacement therapy is also increased due to increase in diabetes and hypertension. In spite of good monitoring and management patients have increased mortality due to cardiac cause. Dyslipidemia plays a major role in the increases the risk of arteriosclerotic cardiovascular disease which is the leading cause of mortality among chronic kidney disease (CKD) patients. This is a comparative study to access the pattern of lipid profile in CKD patients on conservative management and hemodialysis compared with normal healthy controls at MES medical college hospital between Jan 2018 to June 2019. Subjects with CKD both on conservative management and haemodialysis were included in the study and age matched control group. Patients with disease affecting the lipid metabolism, pregnancy and patients on drugs causing lipid abnormality were excluded. Lipid profile was collected from eligible patients and controls. In the present study the mean age of the study group and control were 51.12 ± 10.97 and 44.66 ± 10.13. In a total of 100 subjects participating in the study, males constituted about 61% of total study population compared with females constituting 39%.In our study dyslipidemia in aspects of elevated levels of TC, TGL, LDL and low levels of HDL were noted. Monitoring and treatment of dyslipidemia helps to decrease mortality in CKD patients.
Keywords: Chronic kidney disease, Hypertriglyceridemia, Lipid profile, Dyslipidemia, Coronary artery disease
Cite this paper: Muhammed Sanoop A. V., Shifa K., Vipindas K., Comparative Study of Lipid Profile in Patients with Chronic Kidney Disease on Haemodialysis / Conservative Management with Control Population, American Journal of Biochemistry, Vol. 9 No. 2, 2019, pp. 17-20. doi: 10.5923/j.ajb.20190902.01.
Article Outline
1. Introduction
- As India is emerging as the capital country for diabetes it’s more important to understand diabetic complication. Diabetic nephropathy leading to chronic kidney disease and need of renal replacement therapy is more common. Chronic renal failure (CRF) is a state which results from a permanent and usually progressive reduction in renal function in a sufficient degree to have adverse consequences on other systems [1]. Chronic kidney disease (CKD) has become a public health problem with a global prevalence of around 8–16% [2,3] and with an estimate of >10% (i.e., >20 million) prevalence in the adult United States population. [4] Data from National Health and Nutrition Examination Survey showed that CKD prevalence among ages 60 and above increased from 18.8% in 1988-1994 to 24.5% in 2003-2006. [5] As the patient with CKD have increasing incidence of cardiac events and leading to the mortality it’s important to understand the facts. [6,7] Dyslipidemia is a well-identified risk factor for atherosclerotic cardiac disease (CAD) in the general population but this relationship as risk factor in CKD should be established in higher levels. With an ever increasing CKD burden worldwide due to increasing incidence of diabetes and hypertension. Treating the modifiable risk factors, like dyslipidemia, becomes an essential component for improving outcomes, prevent cardiac event and mortality. Hence we intent to study the pattern lipid profile in patients with CKD in all stages including patients on haemodialysis /conservative management and compare with the age matched control group in south Indian population.
2. Materials and Methods
2.1. Study Design
- This was a cross-sectional observational study.
2.2. Study Location
- The study was done in MES medical college hospital in the department of biochemistry. This study was conducted in 100 patients with CKD in all stages with patient on conservative management and on haemodialysis. Age matched 100 healthy persons were selected as control group. All the patients in this study group were selected from the Department of Medical records/dialysis unit in MES medical college hospital, during Jan 2018 to June 2019. The controls were selected from those who were accompanying the patients and patients reporting to OPD for other consultation.Inclusion Criteria: All patients between the age group of 20 to 70 were selected in the study with established diagnosis of chronic disease with radiological and biochemical evidence. Patients on conservative management and haemodialysis were included in the study. Subjects with diabetes and hypertension included as it’s the most common causes of CKD. Inclusion Criteria for Controls Normal healthy patients who were age and sex related to patients were included as controls with no evidence of any previous renal problems.Exclusion Criteria: Patients with acute renal failure, nephrotic syndrome, liver disease, Cushing’s, or other metabolic disorder were not included in the study. The subjects who are on drugs affecting lipid metabolism such as β-blockers, statins, and oral contraceptive pills were not included. Pregnant Female patients were not included. Patients with diagnosis of cardiac disease were also excluded. All the subjects included in the study were obtained informed consent and after obtaining detail history, clinical examination subjects was investigation for lipid profile.Assessment of lipid profile was done by the method of instrument 1467-VITROS 5600 (dry slide) machine was used.
3. Results
|
|

|
4. Discussion
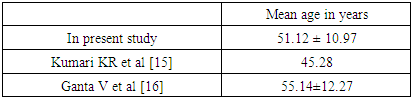
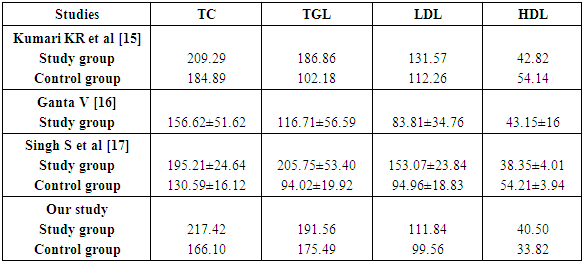
- Coronary artery disease (CAD) is leading cause of mortality and morbidity in patients with mild to moderate chronic kidney disease (CKD) and end stage renal disease (ESRD). In a study done by Hallan SI et al, demonstrated that cardiovascular mortality is higher in young age between 25-34-year-old ESRD patients compare to same age general healthy population [8]. In a retrospective cohort study done by Chertow GM et al identified that the progression of mild to moderate CKD over five years was less when compared to the same patients had more incidence of coronary events leading to high mortality. [9] An independent risk factor for progression of CKD is identified as dyslipidemia based on various evidences. There are multiple mechanisms involved which provide extensive evidence for the processes involved in lipid induced kidney damage. The most prevalent lipid abnormalities which have been noted in chronic kidney disease are hypertriglyceridemia and decreased HDL concentration. The LDL levels are usually found to be normal or increased. Hypertriglyceridemia is evident in various studies in Western studies and recent Indian studies by Gupta DK, Das BS and Bagdae J [10,11]. Elevated triglyceride levels are due to impaired activity lipoprotein lipase (LPL) and direct inhibitory effect of various uremic ‘toxins’ on the enzymes involved in lipid metabolism represent the most important pathophysiological mechanisms underlying the development of hypertriglyceridemia in renal failure [12]. Chan MK et al, also found hypertriglyceridemia was the major abnormality in their studies [13]. Hypertriglyceridemia represents an early feature of renal failure. Different studies identifies low HDLC levels also an independent risk factor for the development CAD among CKD in the Framingham offspring study. Several mechanisms are involved in low HDL levels, which is usually an indication of impaired reverse cholesterol transport. Thus, uremic patients usually exhibit decreased levels of apolipoprotein AI and AII (the main protein constituent of HDL). Reduced activity of LCAT (the enzyme responsible for the esterification of free cholesterol in HDL particles) as well as increased activity of cholesterol ester transfers protein that facilitates the transfer of cholesterol esters from. [14]With the above aspects our studied aimed to establish the evidence in the south Indian population. In the present our observations we noted are as follows:The age distribution of the subject’s ranged between 20-70 years of age. In the present study the mean of the study group and control were 51.12 ± 10.97 and 44.66 ± 10.13.
|
|
|
5. Conclusions
- In our study the importance of dyslipidemia an isolated risk factor to develop CAD in CKD patients. So with the above evidence we state it’s more important to monitor and strict desired levels of lipids to be maintained in CKD patients to prevent mortality due to CAD.
6. Limitations
- 1. Small study group 2. Multicentre approach will give better results 3. Other co morbid and risk factors not described in detail4. Aetiology of CKD not given importance
7. Abbreviations
- CKD - Chronic kidney disease,CAD - Coronary artery disease,TC - Total Cholesterol, TGL – Triglycerides,LDL - Low Density lipoprotein, HDL - High Density Lipoprotein