-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Biochemistry
p-ISSN: 2163-3010 e-ISSN: 2163-3029
2018; 8(2): 40-44
doi:10.5923/j.ajb.20180802.03

A Comparative Study of Biochemical Markers of Myopathy in Hypothyroid and Euthyroid Females
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAshok Vanangamudi1, Divya Ramanathan2
1Assistant Professor, Department of Biochemistry, Government Medical College, Palakkad, Kerala, India
2Assistant Professor, Department of Physiology, Government Medical College, Palakkad, Kerala, India
Correspondence to: Ashok Vanangamudi, Assistant Professor, Department of Biochemistry, Government Medical College, Palakkad, Kerala, India.
| Email: |  |
Copyright © 2018 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background and objectives: Hypothyroidism affects the skeletal muscle causing myopathy and elevation of muscle enzyme levels in serum. The aim of the study was to study the correlation between markers of myopathy and thyroid hormones among hypothyroid patients and comparing it with normal healthy controls. Materials and Methods: This was a hospital based case control study which included 50 hypothyroid female subjects and 50 normal healthy euthyroid female subjects of 30-60 years of age. Serum freeT3, Serum freeT4 and Serum TSH was determined by chemiluminescent immunoassay method. Serum creatine kinase and Lactate dehydrogenase was determined by a semi-automated analyzer. The data analysis was carried out using SPSS for windows 11.5 software. Results: The mean values of TSH, Creatine kinase (CK) and Lactate dehydrogenase (LDH) were significantly increased in patients with hypothyroidism in comparison with the controls (p<0.05). CK and LDH was found to be positively correlated with TSH. Regression analysis with TSH as a dependent variable showed a linear relationship with CK and LDH among the cases. Discussion: The results of our study revealed that hypothyroidism can cause significant increase in Creatine kinase and Lactate dehydrogenase activity. Creatine kinase can be used as a better biochemical marker of assessing muscle damage in hypothyroidism.
Keywords: Hypothyroidism, Myopathy, Creatine kinase, Lactate dehydrogenase
Cite this paper: Ashok Vanangamudi, Divya Ramanathan, A Comparative Study of Biochemical Markers of Myopathy in Hypothyroid and Euthyroid Females, American Journal of Biochemistry, Vol. 8 No. 2, 2018, pp. 40-44. doi: 10.5923/j.ajb.20180802.03.
Article Outline
1. Introduction
- Thyroid dysfunction is one of the most common endocrinology disorders. Thyroid gland synthesizes hormones which has a significant role in control of basal metabolic rate, general body metabolism, growth and tissue differentiation. Abnormalities of these hormones involve many organ systems producing various clinical signs and symptoms. Thus the confirmation of a diagnosis of thyroid disorder depends largely upon biochemical parameters [1].Thyroid hormones stimulate calorigenesis in muscle and increases muscle sensitivity to circulating catecholamines [2]. Hypothyroidism affects the skeletal muscle causing myopathy and elevation of muscle enzyme levels in serum [3-5]. This increase results from leakage of the enzyme from muscle cells, which is related to the alteration in sarcolemma membrane and the subnormal body temperature accompanying hypothyroidism [6].The present study was performed to evaluate the effect of hypothyroidism on muscle functions and to find the correlation between hypothyroidism and myopathy markers.Aims and objectives1. Evaluation of myopathy markers in patients with hypothyroidism and comparing it with normal healthy controls.2. To study the correlation, among markers of myopathy and thyroid hormones among hypothyroid patients.
2. Materials and Methods
- This was a hospital based case control study and was conducted in the Department of Biochemistry at Sri Manakula Vinayagar Medical College and Hospital (SMVMCH), Pondicherry. An informed consent was obtained from both the cases and the controls. Sample and Sample size: 50 normal healthy euthyroid female subjects of 30-60years of age. 50 hypothyroid female subjects of 30-60 years of age.Sampling: A representative sample of local population comprising of 50 subjects aged 30-60 years were selected from1. Hypothyroid patients attending medicine OPD in SMVMCH.2. Normal healthy euthyroid subjects were attendants of patients, workers in SMVMCH. Inclusion criteriaCases: The patients who were diagnosed hypothyroid in the outpatient and inpatient ward of Department of Medicine based on the thyroid and clinical profile.Controls: subjects with normal thyroid status.Exclusion criteria1. Patients with any known muscular disorders, cardiovascular diseases, hypertension, diabetes mellitus or any other systemic medical illness.2. Patient on drugs like antiarrhythmic agents, β blockers, lithium, fibrates, phenothiazine, steroids, statins.Sample collectionThree ml of whole blood were collected from the cases and controls after overnight fasting with dry disposable syringe by venipuncture under all aseptic precautions. Then serum was separated after subjecting the collected blood to centrifugation at 2500 rpm for 5min. Serum was divided into two aliquots. One aliquot was used for thyroid function tests (TSH, Free T3, Free T4) and the another immediately used for analysis of Creatine Kinase (CK), Lactate dehydrogenase (LDH).Estimation of Thyroid function1. Serum freeT3 (normal range 1.4-4.2 pg./dl) was measured by competitive analogue immunoassay method using standard kits obtained from Siemens Healthcare Diagnostics Ltd on a Immulite fully automated analyzer from Siemens. 2. Serum freeT4 (normal range 0.8-2.0 ng/dl) was measured by solid phase enzyme labeled chemiluminescent competitive immunoassay method.3. Serum TSH (normal range 0.3-6.1 µIU/ml) was measured by solid phase two site chemiluminescent immunometric assay method. Estimation of Myopathy markersSerum creatine kinase (normal range 25-190IU/L) and Lactate dehydrogenase (normal range 225-450IU/L) were determined by a semi-automated analyzer Microlab 300 from Merck Diagnostics using standard kits supplied from LabKit and Raichem. Statistical analysisThe results were expressed as mean ± standard deviation. The data analysis was carried out using SPSS for windows 11.5 software. Comparison of parameters between hypothyroid subjects and normal healthy controls was done with student-t test. Pearson’s correlation was applied to test for association between continuous variables. A linear regression analysis was performed with TSH as a dependent variable to show the relationship with creatine kinase and LDH among the cases. A p value <0.05 was considered statistically significant.
3. Results
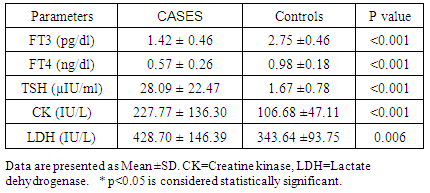
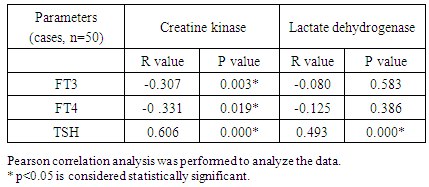
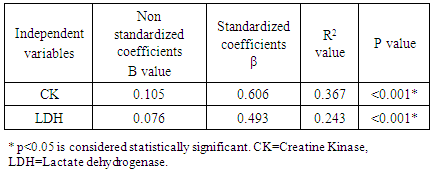
- The results were presented as mean ± standard deviation in table 1. Table 1 summarizes the descriptive statistics of thyroid profile and myopathy markers in hypothyroid group and the control group. The mean values of TSH were significantly increased in patients with hypothyroidism in comparison with the controls (p<0.05). Creatine kinase and Lactate dehydrogenase were significantly increased in patients with hypothyroidism in comparison with the controls.Table 2 shows the correlation of thyroid hormones with Creatine kinase and Lactate dehydrogenase. Creatine kinase is found to be positively correlated with TSH and negatively correlated with FT3 and FT4. Lactate dehydrogenase is found to be positively correlated with serum TSH levels.Regression analysis with TSH as a dependent variable showed a linear relationship with creatine kinase and LDH among the cases. (Table 3). Figure 1 and Figure 2 shows the regression curve of Creatine kinase and Lactate dehydrogenase with TSH respectively.
|
|
|
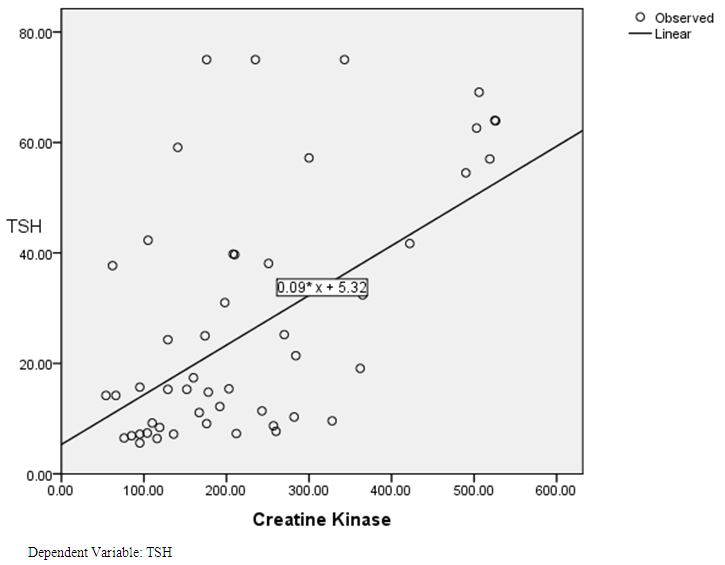 | Figure 1. Linear regression analysis between TSH and Creatine Kinase levels among the cases |
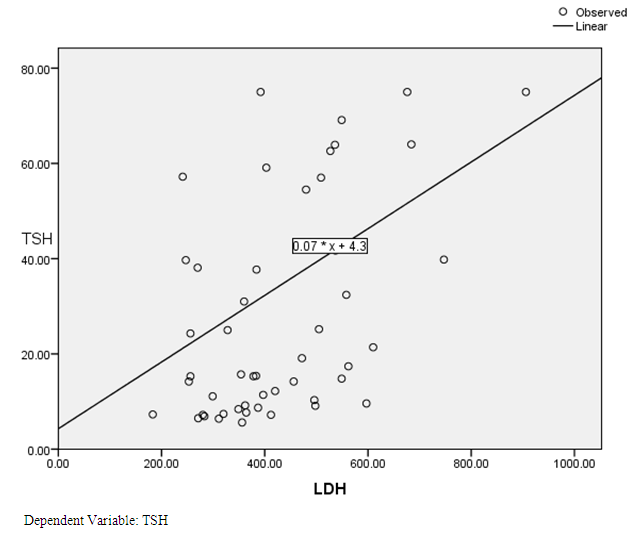 | Figure 2. Linear regression analysis between TSH and Lactate Dehydrogenase (LDH) levels among the cases |
4. Discussion
- Abnormalities of thyroid function can cause a wide spectrum of muscle disorders. Thyroid hormones stimulate calorigenesis in muscle, increase muscle demand for vitamins, and enhance muscle sensitivity to circulating catecholamines. Creatine kinase (CK) is a cytoplasmic and mitochondrial enzyme with extensive tissue distribution [7]. Creatine kinase activity is greatest in striated muscle, brain and heart tissue. In spite of the wide tissue distribution of creatine kinase, it is considered as muscle specific enzyme with clinical utility in the detection of acute or chronic disorder of muscle [8]. Myopathy was a frequent complication of hypothyroidism and hypothyroid patients have frequent muscle complaints. The hypo metabolic state of hypothyroidism can cause a reduction in glycolysis and oxidative phosphorylation thus reducing adenosine triphosphate concentration beyond a critical limit. Proximal muscle weakness, specifically affecting the legs, muscle pains or cramps and delayed tendon jerk relaxation are the commonest feature of hypothyroid myopathy [9]. Skeletal muscle is affected by hypothyroidism more profoundly in cases of overt hypothyroidism as compared to subclinical hypothyroidism [16]. The clinical diagnosis of hypothyroidism should be considered in patients with unexplained persistent elevations of serum creatine kinase [10].The results of our study revealed that hypothyroid patients have significantly higher serum Creatine kinase and Lactate dehydrogenase activity as compared with the controls. This elevation may be due to the skeletal muscle involvement in hypothyroidism. However clinical muscular symptoms were not usually the chief compliant at presentation in hypothyroid patients.Various mechanisms have been proposed as causing elevated creatine kinase activity in hypothyroidism although these mechanisms may have varying influence at different stages of the disease. The increase results from leakage of enzyme from muscle cells which is related to the subnormal body temperature accompanying hypothyroidism and also to the decrease in enzyme clearance. The alteration in sarcolemma membranes can cause increase cell permeability and the leakage of creatine kinase from cells. Another possibility is reduced turnover of creatine kinase because of hypothyroidism allowing serum activities to rise generating a marked release of creatine kinase through the altered sarcolemma membranes [5, 6].In our study 64% of hypothyroid patients had elevated creatine kinase levels and 44% of hypothyroid patients had elevated Lactate dehydrogenase levels. These findings are in accordance with those of other studies, which report a 43% to 97% elevation of serum creatine kinase and 37% elevation of LDH in hypothyroidism [11-15]. Creatine kinase levels in hypothyroid subjects have inverse relationship with FT3 and FT4 and a positive correlation with TSH. Lactate dehydrogenase levels in hypothyroid subjects have a positive correlation with TSH. The results were similar to other studies which showed positive correlation between Creatine kinase and TSH and a negative correlation between FT3 and Creatine kinase in hypothyroid patients [16, 17]. A marked increase in TSH is associated with increase in serum Creatine kinase and Lactate dehydrogenase levels suggesting that the severity of hypothyroidism increases Creatine kinase and Lactate dehydrogenase levels. Among Creatine kinase and Lactate dehydrogenase, Creatine kinase is found to be correlated with TSH, FT3 and FT4 whereas Lactate dehydrogenase is found to be significantly correlated with TSH alone. Creatine kinase was found to be the best indicator of hypothyroid myopathy since they are sensitive for the early detection of muscle involvement due to metabolic disorder and is closely related to the metabolic condition of the patients [11].Linear regression analysis also showed a linear relationship between TSH and Creatine kinase and also between TSH and lactate dehydrogenase. This indicates that TSH can be used to predict changes in muscle enzymes (CK and LDH) in patients with psoriasis.
5. Conclusions
- From the present study, it is evident that hypothyroidism can cause significant increase in Creatine kinase and Lactate dehydrogenase activity, which indicates that these can be used as parameters for screening hypothyroidism. Creatine kinase can be used as a better biochemical marker for assessing muscle damage in hypothyroidism. A large scale study is warranted to further validate the findings of the present study.
ACKNOWLEDGMENTS
- We are grateful to Sri Manakula Vinayakar Medical College and Hospital for providing facilities to perform this study.