-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Biochemistry
p-ISSN: 2163-3010 e-ISSN: 2163-3029
2018; 8(1): 13-17
doi:10.5923/j.ajb.20180801.03

Serum Human Chorionic Gonadotropin as a Biochemical Marker of Adverse Pregnancy Outcome in Severe Preeclampsia
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLShahid A. Mujawar1, Vinayak W. Patil1, Rekha G. Daver2
1Department of Biochemistry, Grant Government Medical College and Sir J.J. Group of Government Hospitals, Byculla, Mumbai, Maharashtra, India
2Department of Obstetrics and Gynecology, Grant Government Medical College and Sir J.J. Group of Government Hospitals, Byculla, Mumbai, Maharashtra, India
Correspondence to: Shahid A. Mujawar, Department of Biochemistry, Grant Government Medical College and Sir J.J. Group of Government Hospitals, Byculla, Mumbai, Maharashtra, India.
| Email: |  |
Copyright © 2018 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Evidences prove that elevated serum human chorionic gonadotropin (hCG) and severity of preeclampsia indicating that secretory dysfunction of placenta play an important role in the pathogenesis of preeclampsia. Therefore serum hCG is useful biochemical markers reflecting the severity of the occurrence of preeclampsia. Objective: The present study was carried out to evaluate the occurrence of association between serum hCG and arterial blood pressure (ABP) in patients with preeclampsia. Material and Methods: This is the case-control hospital based study carried in the Grant Government Medical College and Sir J.J. Group of Government Hospitals, Mumbai. Fifty preeclamptic patients from gynecology ward were studied for estimation of serum hCG over a period of October 2007 to June 2010. Serum hCG determined by means of Immulite 1000 analyzer. Results: The statistical analysis of study group of preeclampsia compared with normotensive control group, showed significant increase in serum hCG concentrations in patients with preeclampsia. Conclusion: The present study found a significant association between serum hCG and ABP as a risk factor for cardiovascular disease (CVD) and secretory dysfunction of placenta in preeclampsia.
Keywords: Human chorionic gonadotropin, Arterial blood pressure, Preeclampsia, Cardiovascular disease, Secretory dysfunction
Cite this paper: Shahid A. Mujawar, Vinayak W. Patil, Rekha G. Daver, Serum Human Chorionic Gonadotropin as a Biochemical Marker of Adverse Pregnancy Outcome in Severe Preeclampsia, American Journal of Biochemistry, Vol. 8 No. 1, 2018, pp. 13-17. doi: 10.5923/j.ajb.20180801.03.
1. Introduction
- Preeclampsia is a serious pregnancy problem distinguished by hypertension, proteinuria with or without pathological edema [1]. It may occur in about 3-10% of all pregnancies. [2, 3] It remain a major cause of perinatal and maternal morbidity and mortality worldwide, because of complications such as preeclampsia, eclampsia, fetal growth retardation, premature birth or abruptio placentae. [4] Even though based on clinical presentation, preeclampsia is considered as a late pregnancy disorder, but the molecular actions leading to its onset seem to occur early in pregnancy. Revealed as a two phase disorder, maternal indications of preeclampsia are considered to be consequences of pre-clinical placental pathology associated with poor placental perfusion, inflammation, ischemia or hypoxia, and trophoblastic injury [5].Human chorionic gonadotropin (hCG) is a two-chain glycoprotein hormone (MW ~37,000) normally found in blood and urine only during pregnancy. [6] Placental tissues are secretes hCG, beginning with the primitive trophoblast, almost from the time of implantation, and serves to support the corpus luteum during the early weeks of pregnancy. [7] A Biosynthesized gold nanoparticle is one of the novel standards for using health industry. Recently gold nanoparticles were used for the detection of tumor, hormones, glucose and other biomolecules in health care services. Higher hCG levels are found in preeclampsia and also detected by using gold nanoparticles [8]. Now enzyme amplified chemiluminescent immunoassay and gold nanoparticle techniques sustained 100% accurate in diagnosis of pregnancy and it may be a good alternative method for urine pregnancy test.According to literature, several researcher showed that elevated serum hCG level can be a diagnostic marker of preeclampsia. These considerable evidence suggests relationship between serum hCG and preeclampsia. [9-11] We therefore studied whether the serum hCG concentration dose correlate with arterial blood pressure (ABP) and might indicate the severity of preeclampsia.
2. Material and Methods
- Design of Study: A prospective comparative case control study. Setting: This study was carried out at Department of Biochemistry, Grant Government Medical College and Sir J.J. Group of Government Hospitals, Mumbai. All participants completed a medical history form and provided informed consent. Study population: Fifty preeclamptic patients in the age group of 18 to 35 years were studied for estimation of serum hCG and ABP over a period of January 2008 to June 2010. Control group consist of 50 healthy normotensive pregnant subjects of identical age without any disease were enrolled. The Institutional Ethical Committee at the Grant Government Medical College and Sir J.J. Group of Government Hospitals, Mumbai, India, approved the study.Inclusion and exclusion criteria: Inclusion criteria for women included in the study were: Patients with symptoms and signs suggestive of preeclampsia supported by laboratory investigations and should not be using any kind of oral contraceptives, anticoagulant drugs, should be non-smokers and non alcoholics were included in the study. Exclusion criteria was: past history of diabetes, systemic or endocrine disorder, chronic infection, chronic renal disease and hypertension, women in the labour pains, were excluded from the study.Blood sample collection: Venous blood samples were collected in test tube with aseptic precautions. After 2 hours of collections sample was centrifuged at 3000 rpm for 5 minutes. Serum was separated and collected in polythene tube with cork. The sera with no sign of hemolysis used for the analysis of hCG.Biochemical Analysis: Serum hCG concentration was measured by solid-phase, two site chemiluminescent immunometric assay. [12] We used fully automated enzyme amplified chemiluminescent immunoassay based Immulite 1000 analyzer. Measurement of these blood parameters by using commercial kits from Siemens Medical Solutions Diagnostics, Los Angeles, CA, USA. Measurement of arterial blood pressure: Blood pressure was measured by the standard sphygmomanometer technique. Patients were allowed to rest for 30 minutes. All measurement taken with the help of Clinician. Hypertension was defined as a systolic blood pressure (SBP) reading greater than 140 mmHg and/or a diastolic blood pressure (DBP) reading greater than 90 mmHg. Statistical AnalysisNumerical variables were reported in terms of mean and standard deviation. Statistical analysis of results was done by normal distribution ‘Z’ test. In this analysis, variables showing p value less than 0.05 and 0.001 were considered to be statistically significant and highly significant respectively. Correlation coefficient (r) was calculated for finding correlation between two biochemical parameters by using Pearson two-tailed analysis.
3. Results
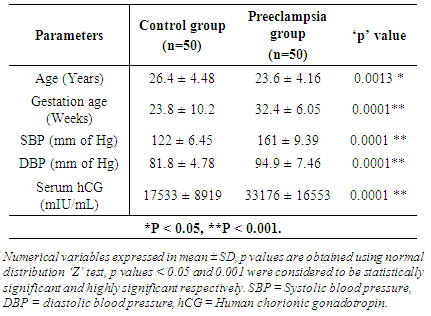
- The demographic details of both study groups are mentioned in table 1. Maternal age was significantly different between the groups (p<0.05). Whereas gestational age, systolic and diastolic blood pressures were significantly higher in preeclamptic groups as compared to normal pregnant women (p<0.0001).
|
|
4. Discussion
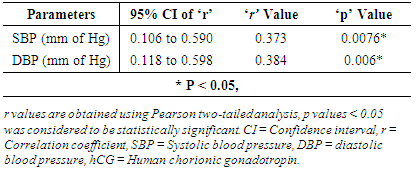
- Our finding suggests that levels of serum hCG were altered in preeclampsia patients than in age-matched normotensive pregnant controls. In preeclampsia patients age, SBP and DBP showed significant different as compared with those of controls. Importance of these parameters has been recognized estimating cardiovascular disease risk factor due to their positive association with hypertension. [13]Serum hCG as a marker of cytotrophoblast differentiation, El-Baradie SMY et al. showed elevated levels of serum hCG in women with preeclampsia and intrauterine growth restriction may identify a placental predisposition to differentiation in vivo. [14] The mean serum hCG level in preeclamptic cases was significantly higher (p<0.001) than the normotensive pregnant cases. This finding showed that secretory dysfunction in preeclampsia. [15] Histopathological study showed by John P et al; focal cellular necrosis in the syncytiotrophoblast and increment in mitotic function with cellular proliferation in the cytotrophoblast during preeclampsia. [16]Yin B, studied 193 normal term women and patients with pregnancy induced hypertension for determination of maternal serum hCG hormones by semi quantitative immunohistochemistry. He found, a strong positive and significant correlation between the maternal serum level of hCG and the immunostained positive syncytiotrophoblasts. Maternal serum hCG was produced mainly from placental syncytiotrophoblasts. Serum hCG and hCG positive cells of the placenta were obviously higher in patients with PIH than those in normal and concluded that abnormal higher hCG level might affect the pathogenesis of PIH. [17] The results of our study are consistent with previous study measured serum hCG concentration in preeclampsia and normotensive pregnant women and found elevated levels of serum hCG preeclamptic cases. [18-23]Positive and significant correlation (r = 0.373, P < 0.05) was observed between serum hCG compared with SBP in preeclampsia. Their 95% confidence interval of correlation coefficient ‘r’ was ranged from 0.106 to 0.590 (figure 1). Correlation between serum hCG and DBP showed positive and significant correlation (r = 0.384, P < 0.05) in preeclampsia. Their 95% confidence interval of correlation coefficient ‘r’ was ranged from 0.118 to 0.598 (figure 2). A study conducted by Gurbuz et al showed that a high serum hCG can be a helpful marker in the diagnosis and management of this disease. [24] These observations and correlation between hCG and arterial blood pressure, support our findings and add to the strength of this information.
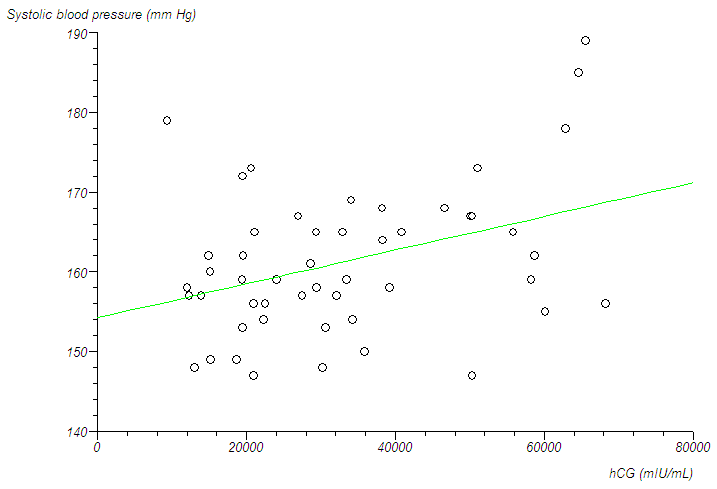 | Figure 1. The correlation between serum hCG and SBP in preeclampsia |
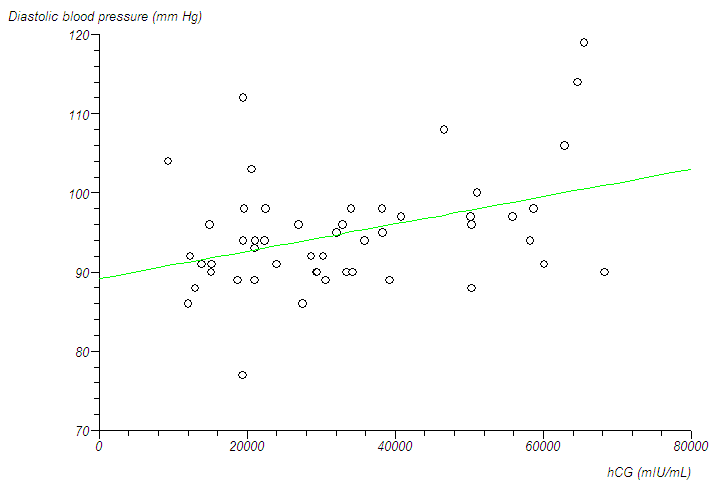 | Figure 2. The correlation between serum hCG and DBP in preeclampsia |
5. Conclusions
- Our study supports a strict relationship between elevated serum hCG and severity of preeclampsia indicating as a risk factor for cardiovascular disease and secretory dysfunction of placenta in preeclampsia. On the other hand, there is an absolute need for large studies designed to answer the question as to whether abnormally elevated serum hCG and arterial blood pressure and are associated with increased risk for cardiovascular disease and secretory dysfunction of placenta in preeclampsia.