-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Biochemistry
p-ISSN: 2163-3010 e-ISSN: 2163-3029
2015; 5(4): 73-76
doi:10.5923/j.ajb.20150504.01
Level of Serum Chromium in Sudanese Type 1 and Type 2 Diabetes Mellitus Patients
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKhalid Mohamed Adam1, Hala Abdalla Elmadni Ibrahim2
1Department of Molecular Biology, Faculty of Medical Lab Sciences, Alneelain University, Khartoum, Sudan
2Department of Clinical Chemistry, Faculty of Medical Lab Sciences, Alneelain University, Khartoum, Sudan
Correspondence to: Khalid Mohamed Adam, Department of Molecular Biology, Faculty of Medical Lab Sciences, Alneelain University, Khartoum, Sudan.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
Background: Chromium is one of the most abundant elements on earth’s crust, it is an essential trace element for proper insulin functioning and blood glucose regulation. The role of the trace element in causing diabetes mellitus was investigated by several previous studies, however, the present study aimed to investigate the effect of the disease on the status of the trace element in Sudanese diabetes mellitus patients. Materials and Methods: Serum chromium level was measured with flame atomic absorption spectrophotometer in blood specimens collected from diabetes mellitus type 1, diabetes mellitus type 2 patients, and apparently healthy control groups. Results: Patients with diabetes mellitus type 2 showed the lowest level of serum chromium level amongst the three study groups, while the control group showed the highest level. No statistically significant difference in the serum chromium level was observed when compared in all study groups according to gender. No significant association was seen between the level of serum chromium in all study groups and both age and duration of the disease. Conclusions: It can be concluded that patients with diabetes mellitus have reduced levels of serum chromium as compared to their healthy counterparts, though it is not quite clear whether low chromium level is the cause or the consequence of the disease.
Keywords: Chromium, Diabetes mellitus, Sudanese, Trace element
Cite this paper: Khalid Mohamed Adam, Hala Abdalla Elmadni Ibrahim, Level of Serum Chromium in Sudanese Type 1 and Type 2 Diabetes Mellitus Patients, American Journal of Biochemistry, Vol. 5 No. 4, 2015, pp. 73-76. doi: 10.5923/j.ajb.20150504.01.
Article Outline
1. Introduction
- Diabetes mellitus is by far, the most common non-communicable disease in Sudan with high morbidity and mortality rates, and prevalence ranges from 2.6% in the rural areas [1] to 3.4% in the urban areas [2]. The disease is emerging as an additional burden to the already economically compromised country, and the incidence rate is increasing rapidly to the level of becoming an epidemic. The intricate relationship between the perturbations in trace elements metabolism and the pathogenesis of diabetes mellitus has allured many clinical researchers [3-8] Many trace elements are essential for proper metabolic functioning of the human body. Their deficiency is believed to be behind many disorders such as anaemia, heart disease and diabetes mellitus [9, 10, 3]. The deficiency of micronutrients such as Zn, Cr, Cu and Mg for instance, have been shown to affect glucose homeostasis causing glucose intolerance, chronic hyperglycemia and thus diabetes mellitus.Chromium is one of the most common elements in planet earth. It is normally found in one of two oxidation states, trivalent Cr (III) and hexavalent Cr (VI); the latter is a known toxin, mutagen and carcinogen [11], while the former is essential for insulin action and proper carbohydrate and lipid metabolism, found in most food and nutrient supplements, and it is of very low toxicity. Trivalent chromium is the most stable form, and exists as inorganic salt or complex with organic ligands such as glucose tolerance factor (GTF) in brewer’s yeast and as low molecular weight chromium-binding peptide (LMWCr) in animal cells [12]. The possible effect of chromium on carbohydrate is believed to be by potentiating the action of insulin [13]. Although the exact mechanism of action is yet to be determined, the possible role of GTF is as carrier of chromium to the chromium-deficient proteins of the cell [14]. While LMWCr is believed to potentiate the insulin response by activating the insulin receptor, the degree of receptor activation depends on chromium ions bound this peptide [15]. Despite the large literature on the role of dietary composition in causing and management of diabetes mellitus, there are relatively few studies on the effect of diabetes mellitus on micronutrient status of the individual, as most of the published studies focused on the role of chromium supplements in management of diabetes mellitus complications, and very few studies with conflicting results discussed the effect of the disease on the micronutrient status [16-18, 10].The aim of this study is to evaluate the serum chromium status in Sudanese diabetes mellitus patients. All participants in this study were carefully selected following a very restrict inclusion and exclusion criteria.
2. Materials and Methods
- A descriptive case control study included 150 participants, divided into 3 groups; Type 1 diabetes mellitus patients (50), Type 2 diabetes mellitus patients (50), and the control group comprised of apparently healthy individuals (50). The study was approved by the ethical committee of faculty of medical laboratory sciences – Alneelain University. An informed verbal consent was obtained from each participant prior to specimen collection. All participants were randomly recruited from Khartoum hospital after a primary random glucose test and HbA1C estimation. Individuals were assign to each of the three groups based on the following criteria for diabetes; HbA1C above 6.5%, random blood glucose ≥200 mg/dl, fasting blood glucose ≥140 mg/dl, while assigning patients to type 1 and type 2 based on the age of disease onset. Individuals were excluded from the study if they suffered from any chronic illness, under medications that affect chromium level, smokers, alcoholics, and leather tanning workers. From all participants two specimens, 3 ml each, were drawn in two different containers, fluoride oxalate for glucose estimation, and plain containers for serum preparation for chromium determination.Plasma glucose was estimated using the glucose oxidase method [19] described by Barharm and Trinder, using commercially available kits from Biosystems (Spain), while the chromium level was determined using flame atomic absorption spectrophotometer method previously described by Kaneko [20].
2.1. Statistical Analysis
- The ANOVA test was used to compare between the three different groups, and the results are presented as mean difference, while associations were assessed with Pearson correlation test. The statistical significance was set at P<0.05. Data were analyzed using Statistical Package for Social Sciences (SPSS.14).
3. Results
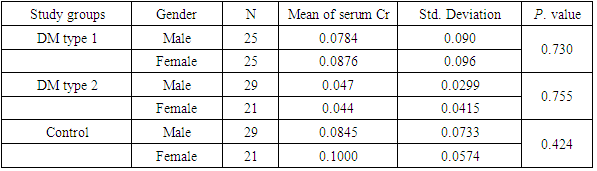
- The results of the present study shows statistically significant difference between the mean serum chromium in DM type 1 patients and type 2 with mean difference 0.036 and P. value 0.009, the mean serum chromium level showed no statistically significant difference between DM type 1 and control group with mean difference -0.008 and P. value 0.563, while the chromium level of DM type 2 showed statistically significant difference when compared to that of control with mean difference -0.044 with P. value 0.002 as shown in table 1.
|

|
|

4. Discussion
- Diabetes mellitus is a group of metabolic diseases characterized by inability of the body to metabolize glucose due to abnormal amount or activity of insulin hormone, which was reported in many studies to be the function of number of trace elements deficiency [21]. A number of studies have reported that chromium supplements enhance the action of insulin and reduce the risk of DM complications development [18]. Chromium activity depends mainly on its valence, with trivalent Cr being the most essential form for glucose metabolism [22-24]. It enhances blood glucose uptake by the cells by stimulating insulin signaling pathway and increasing the number of glucose transporter in the cell membrane [25]. The trace element deficiency is believed to lead to glucose intolerance, and thus to diabetes related complications [4]. Metabolism of micronutrient Cr was one of many believed to be altered by DM [26]. The findings of the present study showed that level of serum chromium in healthy control is the highest among the three study groups, as indicated by the negative mean difference, while patients with DM type 2 showed the lowest level, this result goes in concordance with the general belief and with the findings of many studies [27-29, 8]. Unlike type 2, DM type 1 is generally insulin dependent and insulin sensitivity not altered, therefore the level of serum chromium is significantly high in type 1 as compared to type 2. Patients with DM type 2 frequently show diminished insulin sensitivity and relative deficiency of endogenous insulin secretion [30, 31] low concentration of insulin in addition to increased glucagon secretion will lead to high rate of hepatic glucose anabolism, thus, elevated fasting blood glucose levels [31] due to increased glucose production in the liver and increased free fatty acids production, this results in hyperglycemia and osmotic diuresis, therefore, increase urine Cr excretion, as reported previously [29] that patients with DM type 2 show abnormally high urine Cr levels. The level of serum Cr of males and females showed no difference in all study groups, these findings are in good agreement with the results of study [4] carried out to determine the level of the micronutrient in different biological specimens, where the difference on serum Cr based on the gender was reported to be between the study groups rather than within the same group.Although serum Cr level showed negative association with age of the subjects in all the study groups, however, this association is of no statistically significant value (P>0.05), this contradict the report [4] that level of serum Cr is associated with the age. The lack of significant association in the present study can be attributed to the fact that all three groups comprised of young to middle aged subjects, where the problems of low absorption, slow cellular uptake, and low metabolic rate, normally associated with older age, seldom encountered. Duration of the disease had no major influence on the level of the micronutrient in both type 1 and type 2 patients, this indicates that serum Cr deficiency is a function of the disease itself, rather than duration of the disease.
5. Conclusions
- Although it is not clear whether the disease lead to serum Cr deficiency, or the low levels of the trace element caused the disease, but it is safe to say that patients with diabetes mellitus have reduced levels of serum Cr as compared to their healthy counterparts. It can also be concluded that in young and middle aged patients, age has no or very little effect on the level of serum Cr level. The results of the present study also suggest that level of the trace element is not influenced by the duration of the disease.
ACKNOWLEDGEMENTS
- We are highly indebted to staff of clinical chemistry department, faculty of medical lab science – Alneelain University, and Khartoum teaching hospital for their never ending help.