-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Economics
p-ISSN: 2166-4951 e-ISSN: 2166-496X
2015; 5(2): 177-182
doi:10.5923/c.economics.201501.21
Determinants of Brand Equity in Private Healthcare Facilities in Klang Valley, Malaysia
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLShishi Piaralal1, Tan Mei Mei2
1OUM Business School, Open University Malaysia
2Marketing Department, Columbia Asia
Correspondence to: Shishi Piaralal, OUM Business School, Open University Malaysia.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
Healthcare services are a necessity for every person in every part of the world. In Malaysia, the government and private hospitals play crucial roles in meeting the needs of the country. The study of brand equity is important to gain a competitive advantage in business, especially in healthcare. The research looked into three determinants that affect brand equity, namely perceived quality, brand loyalty and brand image. A quantitative research was conducted for numerical measurement and analysis. The nonprobability sampling method of convenience sampling was used to study behavior of consumers. 200 respondents were selected as the sample size and data was collected through a self-administered questionnaire. Based on the completed 123 respondents who had experienced outpatient treatment and services in private healthcare facilities in the Klang Valley, the results of the research indicate that there is a strong relationship between brand equity and perceived quality, brand loyalty and brand image. The limitation and recommendation for future research is presented at the end of the paper. The research also attempts to bridge the gaps that exist from poor facilities and services rendered by these facilities that will result in the drop of brand value for the organization.
Keywords: Brand equity, Perceived quality, Brand loyalty, Brand image, Private healthcare facilities, Government hospitals
Cite this paper: Shishi Piaralal, Tan Mei Mei, Determinants of Brand Equity in Private Healthcare Facilities in Klang Valley, Malaysia, American Journal of Economics, Vol. 5 No. 2, 2015, pp. 177-182. doi: 10.5923/c.economics.201501.21.
Article Outline
1. Introduction
- The healthcare industry is a thriving industry in the world, and also in Malaysia. People in general will require healthcare services at one time or another in their lives. Services can range from general wellness, health screenings, deliveries of babies, specialist care, and emergency care to chronic illnesses care. And it is important that the hospitals offering these services be concerned about the quality of the services provided enabling the facility to sustain its business especially in obtaining brand equity.Organizations that are concern about the health of the business have always placed importance of understanding the internal and external environment. Knowing what the others in the same industry are practicing is often a benchmark for organizational improvement. What sets an organization apart from another is the unique selling proposition or competitive advantage. Having this competitive advantage and knowing how it can help a business will often bring additional profits and larger market share to the organization. And when an organization is successful in increasing its market share, it will generatehigher value and perception in the minds of consumers. The value of the organization is referred as brand equity.Various researches have concluded with many determinants or antecedents to brand equity. Aaker (1991) studied five factors; perceived quality, brand loyalty, brand association, brand awareness and other proprietary assets, that affect brand equity. He developed the brand equity model from the five factors mentioned. Chahal and Bala (2012) later conducted a research on brand equity in India that looked at three factors of which two were similar to Aaker’s perceived quality and brand loyalty. Brand image was the additional factor added into the research for the healthcare sector in India. Guided by the study done by Chahal and Bala (2012), this paper will explore the three determining factors; perceived quality, brand loyalty and brand image for private healthcare facilities in Klang Valley, Malaysia. Organizations develop brands as a way to attract and keep customers by promoting a lifestyle, value and image. With the mention of a brand, whether a product or a service such as Coca Cola, Starbucks, Apple, Google, etc., an image would come to the mind of the consumer. These brands have been successful in creating value for the companies and are recognized worldwide for its products and services. The perceptions created in the minds of consumers are so strong that substitute brands will need longer time to penetrate the market and consumers’ pockets.Because of the proper allocation of financial resources and organizational planning that goes into marketing the brand, the acceptance among consumers is relatively easy therefore increasing the value of the company. Erden et al (1999) refers to this value creation as brand equity. Yoo et al (2000) further researched on the relationships that marketing mix elements have on brand equity. The study explores the marketing mix elements such as product (and service), price, promotion, and place that are related to the dimensions of brand equity.Malaysia operates a two-tier healthcare system (government and public hospitals). Private hospitals serve to complement the demand for healthcare treatments for the population. With the government’s encouragement for health tourism, the expectations of private hospitals to provide world class service is also priority. In doing so, it is more important that private hospitals focus on exceeding patients’ expectations and have in place strategies to improve its brand equity. The basic tier provides the basic and necessary medical needs, while the secondary tier exists for those who are able to purchase better treatments and want quicker access to healthcare service. The private hospitals belong to the secondary tier healthcare system. In other words, there are government and private hospitals in the country to cater to individual needs of the population. The building of brand equity would assist the public in decision making when considering healthcare in the country.
2. Literature Review
- Brand equity is recognized as a key strategic business asset of a company in contemporary marketing theory and practice. Many researchers have offered different viewpoints on variables and drivers that influence brand equity. For the past two decades, researchers such as Farquhar (1989) and Aaker (1991) have discussed to a great extent the many definitions approaches to the brand equity concept.Aaker (1991) developed the brand equity model that consist of perceived quality, brand awareness, brand association, brand loyalty and other proprietary brand assets. The combination of the factors will enable a company to achieve high brand equity. Keller (1998) developed the Customer-Based Brand Equity (CBBE) model. Keller’s model is to build the right type of experiences around your brand, so that customers have specific, positive thoughts, feelings, beliefs, opinions, and perceptions about it. When there is strong brand equity, customers will purchase more, recommend the brand to others, become loyalists and are less likely to lose them to competitors.The theory of planned behavior (TPB) developed by Azjen (1991) with three significant factors; attitude, subjective norm and perceived behavioral control, is complemented by Keller’s CBBE model to determine customer purchase intention. Strong brand equity is a result of customer having a positive attitude towards a brand, the positive word of mouth referrals from family, relatives and friends who recommend the brand. Both the attitude and behavioral norms would be favorable in customer purchase intention. This research was done based on the social adaptation theory whereby assimilation and accommodation changes consumer attitude. Advertising also affects the consumer purchase intention.There are two major approaches to brand equity; a customer-based approach that is based on market perception, behavioral intention and attitudes of (e.g. Aaker, 1991; Keller, 1993; Sriram et al., 2007). The second approach is based on financials whereby a company’s actions and marketing efforts are used to enhance the brand value (e.g. Ailawadi et al., 2003; Sriram et al., 2007).Atilgan et al. (2005) states that there are limited number of quantitative research that examines brand equity constructs which are based on solid empirical data despite numerous conceptual definitions and models of brand equity. In order to investigate further, it is necessary to research the drivers and sources of brand equity in an industry-specific context, and in this study, the healthcare industry.As with all organizations, service is one of the biggest determining factors for customers when selecting products or services. Patients nowadays are viewed as customers and medical service providers are required to understand and act accordingly to customers’ expectations during the service encounter. Keller and Lehmann (2006) have argued that a brand represents its influence at three primary market levels – customer, product and financials. When private hospitals provide quality service, patients will develop a good impression on the capability of private healthcare thereby raising its brand equity.Even though Aaker (1991), Keller (1993) and Sriram et al. (2007) values brand equity using customer-based approach, the attitudes and behavioral actions of consumers do not convert customer value into financial value. Mizik and Jacobson (2008) asserts that “mere assessment of brand attributes is insufficient”, because customer-based attributes must be linked to the financial value of the brand.Experience is one of the indicators of service performance and results in better marketing and financial outcome for the firm (Grewel et al., 2009). A memorable and consistent experience with a brand creates strong brand equity, especially in healthcare. Building strong brand equity is essential for differentiating a firm’s offerings from its competing brands (Yoo et al., 2000).Brand perceptions are attributes in consumer memory that are linked to the brand name (Keller 1993). Gardner and Levy (1955) have researched on this which articulated that the brand was more than just the sum of the functional qualities it offered. Brand perception was also considered to be a key aspect of brand equity (Aaker 1991, 1996; Zeithaml, 1996). Service quality is defined as how well the service meets or exceeds the customers’ expectations on a consistent basis (Parasuraman et al, 1985). In a separate study conducted in Australia by Gill and White (2009) concluded that perceived quality was a proven construct in the adoption of healthcare services.Brand loyalty is associated with service loyalty, purchase intention, word of mouth, price sensitivity and complaining behaviors, which are the main determinants of brand loyalty drawn from the studies of Bloemer et al. (1999) and Kim et al. (2003). Atilgan et al. (2005) states that brand loyalty is considered the strongest path leading to brand equity. Aaker (1991) defines this as the attachment of a consumer towards a brand even when an organization makes changes in the price or other features.Brand image has been defined as cognitive and affective based perceptions consumers have towards a brand (Dobni & Zinkham, 1990). It also consists of symbolic and functional beliefs about the brand (Low & Lamb, 2000). Keller (1993) earlier identified brand image as an association consumers’ hold in their memories regarding a product. Grewel et al (1998) also found a positive relationship between brand image and the level of consumer perception of a product’s quality. A positive relationship has also been found between brand image and the level of brand loyalty displayed by consumers (Yoo et al, 2000). Burmann et al. (2008) also said that brand image is an important determinant of a buyer’s behaviour.
3. Research Methods
- The research framework that guided this research is presented in Figure 1 below. It involves three independent variable; perceived quality, brand loyalty and brand image, and one dependent variable; brand equity.
3.1. Research Design
- The current study had utilized a quantitative research design to address the research questions and objectives. A quantitative method of study was employed to determine the satisfaction level of outpatient services provided by private healthcare facilities in Malaysia.A self-administered questionnaire design was utilized to obtain the data for this research. Convenience sampling was utilized for this research as it is the most convenient and because characteristics of sample are identified, the sampling accuracy will be much higher. For the purpose of this research, a structured questionnaire that follows the quantitative paradigm consisting demographics and item constructs (47 questions) was used to collect data. Data from different groups were obtained to maximize analysis on the similarities and differences that are present. Most item constructs were adapted from Chahal and Bala (2012). Perceived quality consists of 20 items, brand loyalty consists of 12 items and brand image and brand equity consist of 2 items each. Items were measured using a 5-point Likert scale (1 is strongly disagree and 5 is strongly agree). There was also an open-ended question for respondents to provide suggestions and feedback that would raise the brand image of the hospital.The survey was distributed to respondents residing in Selangor and Wilayah Persekutuan. Due to the proportion of urban population that are focused in the Klang Valley, the targeted group of respondents was suitable in line with the cluster of private healthcare facilities that are also located primarily in the Klang Valley area.
3.2. Analysis and Interpretation
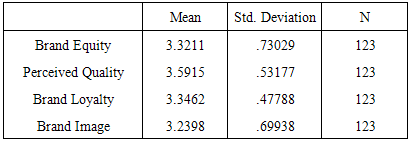
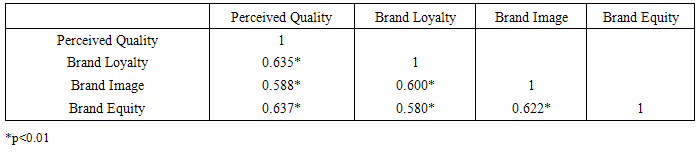
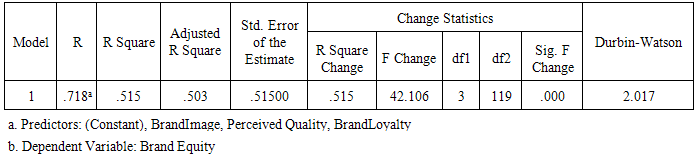
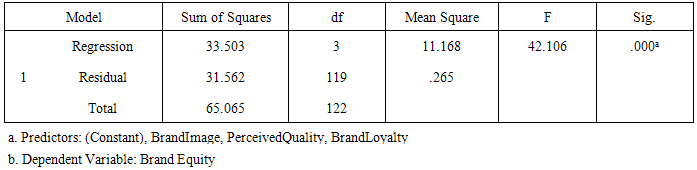
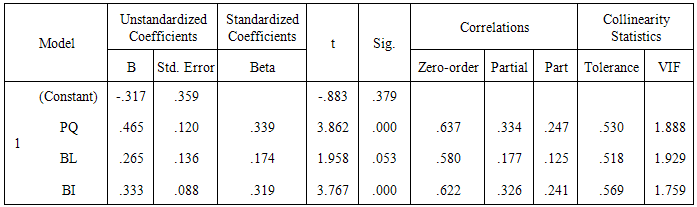
- A total of 200 survey questionnaires were distributed, and 130 respondents returned the questionnaire for a response rate of 65%, of which 123 respondents were complete, providing an effective response rate of 61.5%.Demographic of respondents made up the following:Gender: 57.7% (71) female respondents, 42.3% (52) male respondents.Ethnicity: 40.7% (50) Malay, 43.1% (53) Chinese, 13.8% (17) Indian and 2.4% (3) are from other ethnics.Age: 22% (27) are between 21 – 30, 43.1% (53) are between 31 – 40, 29.3% (36) are between 41 – 50 and 5.7% (7) are ages 51 and above.Marital status: 27.6% (34) are single, 62.6% (77) are married, 5.7% (7) are divorced and 4.1% (5) are widow / widower.Education level: 6.5% (8) are SRP/PMR/SPM holders, 16.3% (20) are STPM / Diploma / A-levels / IB holders, 54.5% (67) are Degree holders and 22.8% (28) are Masters / PhD holders.Occupation: 30.1% (37) are Executives, 37.4% (46) are Managers, 8.9% (11) are Management level, 8.1% (10) are Professionals and 15.4% (19) are retirees or housewives.Income level: 40.7% (50) earns below RM5,000, 20.3% (25) earns between RM5,001 and RM7,000, 8.1% (10) earns between RM7,001 and RM9,000, 13% (16) earns between RM9,001 and RM11,000, 4.1% (5) earns between RM11,001 and RM13,000, 11.4% (14) earns RM13,001 and above, and 2.4% (3) do not have any monthly household income.123 respondents provided multiple reasons for the question; 54 respondents stated previous experience as the main reason for the hospital selection, followed by 34 respondents for convenience and 25 respondents selected the hospital because of Doctor’s specialty. Company insurance was the fourth top reason with 21 respondents followed by 17 respondents who selected the hospital for its nursing care. 14 respondents returned for follow-up visit, while 12 respondents each selected hospital environment and caring doctors as reasons. 9 respondents each selected family’s recommendation and ease of finding parking for selecting the hospital, while only 8 respondents selected based on doctor’s recommendation. There was no respondents who selected promotional voucher.For treatments sought from hospitals, 39 respondents cited general screening as top reason, followed by women’s health concerns from 27 respondents. 24 respondents were seeking paediatrician services while 13 respondents required specialists services. 10 respondents visited the hospital for pre-employment check-up while 4 respondents were seeking diabetes treatments. 2 respondents each visited for emergency care and stress related issues, and 1 respondent sought for men’s health issues.Frequency of treatments 63.4% (78) frequented the hospital 1 – 2 times per year, 26% (32) frequented 3 – 5 times per year, 9.8% (12) frequented 6 – 9 times per year and 0.8% (1) frequented the hospital over 10 times per year.Multiple regression was conducted to test the direct relationship between independent and dependent variables. The analysis was used to examine the impact of the three determinants of brand equity (perceived quality, brand loyalty and brand image). Table 1 and 2 reflects the descriptive statistics and inter-item correlation matrix of all independent and dependent variables. Table 3 depicts the results of regression procedure where all dimensions of brand equity proposed regressed on dependent variable. The results shows 51.5% contribution of the factors to higher value of brand equity.
|
|
|
|
|
4. Implication of Study
- There are many challenges that hospitals may face due to the changing needs of patients. The determinants of brand equity; perceived quality, brand loyalty and brand image, will require constant monitoring and updating to keep up with patient needs. Since the coefficient result of this study identified perceived quality as the highest contributor to brand equity, hospitals need to consistently ensure the quality of services provided are at optimum level.With the increased exposure and added access to information, patients are also savvy in realizing the availability of other providers in the market, and would not hesitate to switch if their needs are met by substitute providers. Without the clear expectations for behavior, responsiveness and communication, the hospital is at risk of spending more time and resources to mitigate effects of patients switching providers.Building a brand identity is often a challenge for organizations. The perception of patients on the hospital services, quality and outcomes are areas that need to be managed and managed well.
5. Discussions
- The research has also revealed crucial information which pertains to the reasons for the hospital selection and types of treatments sought from the hospitals. The information would serve well for hospital management to continuously monitor the patient experience in order for them to return. A quality assurance team should conduct frequent audits to ensure procedures and processes are followed. For marketers, this information would allow them to design attractive screening packages, women’s wellness packages and also incentives for parents to bring children for paediatrician routine follow-ups.This research has seen the three influential factors of brand equity being studied. The relationship between the three independent variables of perceived quality, brand loyalty and brand image cannot be denied on having a combined influence on brand equity.The perception of quality among patients centered on service. However, the condition of facility and medical equipment are also indicators of quality for them. The major issue with hospitals in the Klang Valley is the shortage of parking space. Due to the limited land resource; patients, families and friends find this a consistent problem they often have to face.The common aspects that healthcare providers are concern with are usually having the right medical team and treating patients. As shown in the results of the survey, there were other aspects of service that were also important to patients such as the registration and discharge process, interpersonal skills of the hospital staffs or the condition or environment of the facility. Without improvement to the processes deemed important to patients would result in negative outcomes. Customer care personnel would need to spend additional time to build the confidence and trust of patients again.
6. Conclusions
- The interest to conduct this study is to have a better understanding among urban Malaysian consumers’ choice of private healthcare facilities. The perception of hospital is important to those seeking treatment, and brand equity is a relevant condition in meeting that perception. The study could be criticized that only three brand equity factors were examined and analyzed. Future research should analyze other factors such as patient value or lifetime value of a patient, patient experiences, patient satisfaction, etc. along with perceived quality, brand loyalty and brand image for a more comprehensive study of brand equity in healthcare.To build a successful brand, companies must be consistent in delivering quality products / services, nurture customer relationships and deliver relevant, meaningful messages. Valuable brand equity is achieved when the brand is consistent in brand management practice.